

Surgical versus clinical staging prior to primary chemoradiation in patients with cervical cancer FIGO stages IIB-IVA: oncologic results of a prospective randomized international multicenter (Uterus-11) intergroup study
- PMID: 33293284
- PMCID: PMC7788482
- DOI: 10.1136/ijgc-2020-001973
Surgical versus clinical staging prior to primary chemoradiation in patients with cervical cancer FIGO stages IIB-IVA: oncologic results of a prospective randomized international multicenter (Uterus-11) intergroup study
Abstract
Objective: Revised staging of patients with locally advanced cervical cancer is based on clinical examination, imaging, and potential surgical findings. A known limitation of imaging techniques is an appreciable rate of understaging. In contrast, surgical staging may provide more accurate information on lymph node involvement. The aim of this prospective study was to evaluate the impact of pre-treatment surgical staging, including removal of bulky lymph nodes, on disease-free survival in patients with locally advanced cervical cancer.
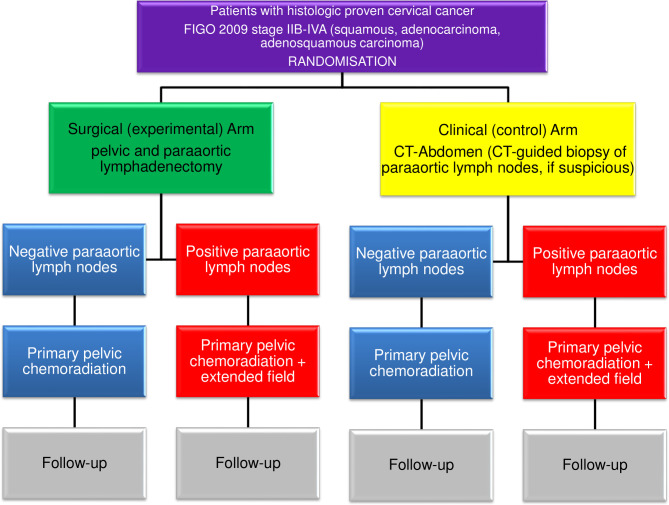
Methods: Uterus-11 was a prospective international multicenter study including patients with locally advanced cervical cancer who were randomized 1:1 to surgical staging (experimental arm) or clinical staging (control arm) followed by primary platinum-based chemoradiation. Patients with histologically proven squamous cell carcinoma, adenocarcinoma, or adenosquamous cancer International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IIB-IVA underwent gynecologic examination and pre-treatment imaging including abdominal computed tomography (CT) and/or abdominal magnetic resonance imaging (MRI). Patients had chest imaging (any of the following: X-ray, CT, or PET-CT). The primary endpoint was disease-free survival and the secondary endpoint was overall survival. An ad hoc analysis was performed after trial completion for cancer-specific survival. Randomization was conducted from February 2009 to August 2013.
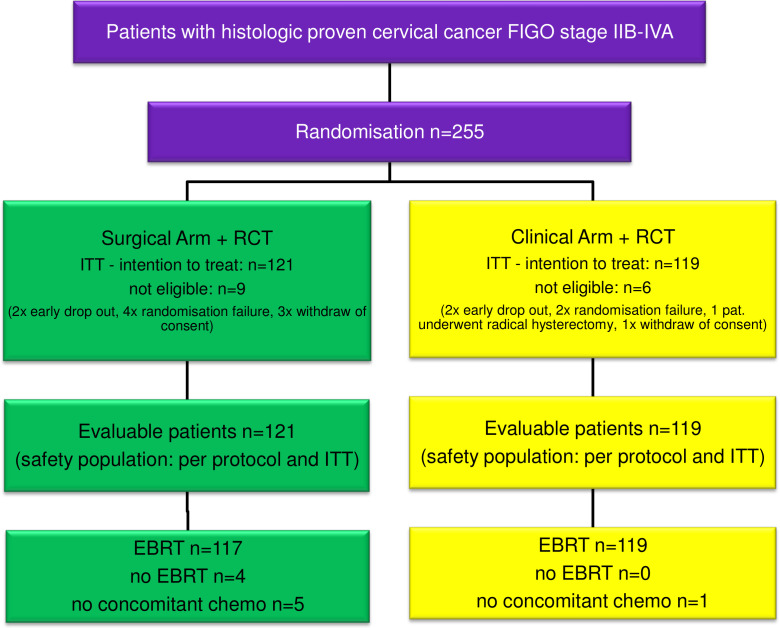
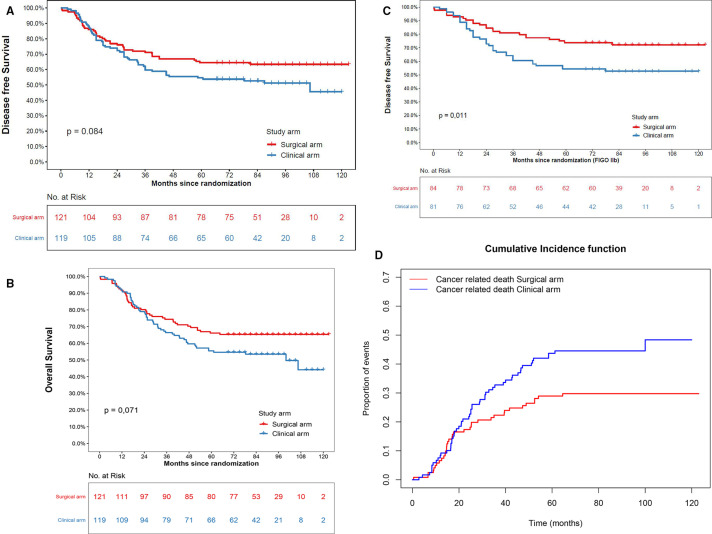
Results: A total of 255 patients (surgical arm, n=130; clinical arm, n=125) with locally advanced cervical cancer were randomized. Of these, 240 patients were eligible for analysis. The two groups were comparable with respect to patient characteristics. The surgical approach was transperitoneal laparoscopy in most patients (96.6%). Laparoscopic staging led to upstaging in 39 of 120 (33%) patients. After a median follow-up of 90 months (range 1-123) in both arms, there was no difference in disease-free survival between the groups (p=0.084). For patients with FIGO stage IIB, surgical staging is superior to clinical staging with respect to disease-free survival (HR 0.51, 95% CI 0.30 to 0.86, p=0.011). In the post-hoc analysis, surgical staging was associated with better cancer-specific survival (HR 0.61, 95% CI 0.40 to 0.93, p=0.020).
Conclusion: Our study did not show a difference in disease-free survival between surgical and clinical staging in patients with locally advanced cervical cancer. There was a significant benefit in disease-free survival for patients with FIGO stage IIB and, in a post-hoc analysis, a cancer-specific survival benefit in favor of laparoscopic staging. The high risk of distant metastases in both arms emphasizes the need for further evaluation.
Keywords: cervical cancer; laparoscopes; operative; radiation oncology; surgical procedures.
© IGCS and ESGO 2020. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Surgical staging, the meaning of life, and other existential ponderings.Int J Gynecol Cancer. 2020 Dec;30(12):1862-1863. doi: 10.1136/ijgc-2020-002174. Int J Gynecol Cancer. 2020. PMID: 33293285 No abstract available.
References
-
- Ramirez PT, Jhingran A, Macapinlac HA, et al. Laparoscopic extraperitoneal para-aortic lymphadenectomy in locally advanced cervical cancer: a prospective correlation of surgical findings with positron emission tomography/computed tomography findings. Cancer 2011;117:1928–34. 10.1002/cncr.25739 - DOI - PMC - PubMed
