

Utility of established prognostic scores in COVID-19 hospital admissions: multicentre prospective evaluation of CURB-65, NEWS2 and qSOFA
- PMID: 33293361
- PMCID: PMC7722817
- DOI: 10.1136/bmjresp-2020-000729
Utility of established prognostic scores in COVID-19 hospital admissions: multicentre prospective evaluation of CURB-65, NEWS2 and qSOFA
Abstract
Introduction: The COVID-19 pandemic is ongoing, yet, due to the lack of a COVID-19-specific tool, clinicians must use pre-existing illness severity scores for initial prognostication. However, the validity of such scores in COVID-19 is unknown.
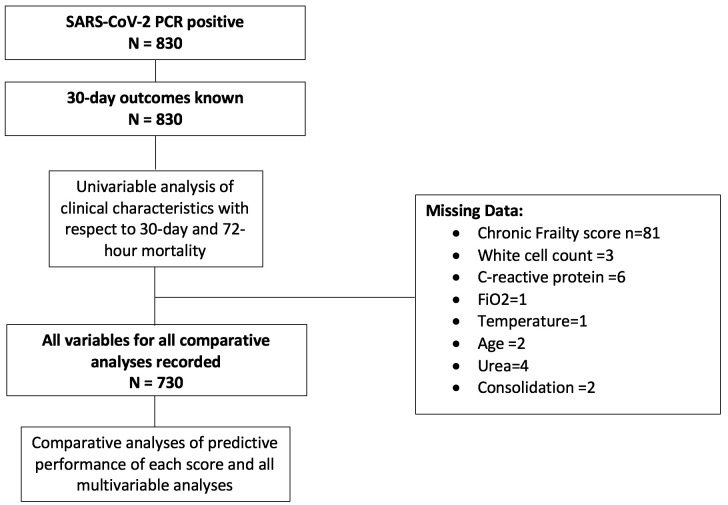
Methods: The North West Collaborative Organisation for Respiratory Research performed a multicentre prospective evaluation of adult patients admitted to the hospital with confirmed COVID-19 during a 2-week period in April 2020. Clinical variables measured as part of usual care at presentation to the hospital were recorded, including the Confusion, Urea, Respiratory Rate, Blood Pressure and Age Above or Below 65 Years (CURB-65), National Early Warning Score 2 (NEWS2) and Quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA) scores. The primary outcome of interest was 30-day mortality.
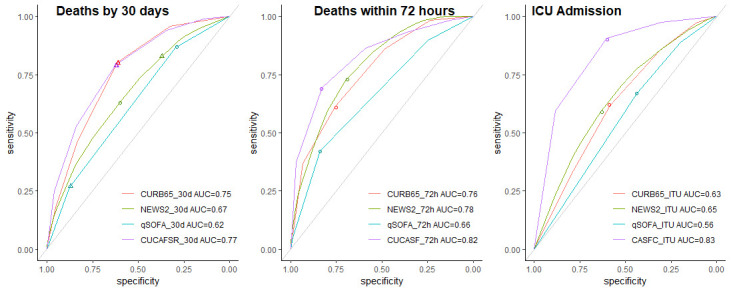
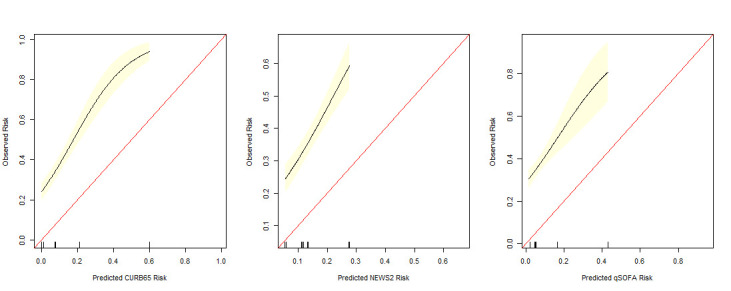
Results: Data were collected for 830 people with COVID-19 admitted across seven hospitals. By 30 days, a total of 300 (36.1%) had died and 142 (17.1%) had been in the intensive care unit. All scores underestimated mortality compared with pre-COVID-19 cohorts, and overall prognostic performance was generally poor. Among the 'low-risk' categories (CURB-65 score<2, NEWS2<5 and qSOFA score<2), 30-day mortality was 16.7%, 32.9% and 21.4%, respectively. NEWS2≥5 had a negative predictive value of 98% for early mortality. Multivariable logistic regression identified features of respiratory compromise rather than circulatory collapse as most relevant prognostic variables.
Conclusion: In the setting of COVID-19, existing prognostic scores underestimated risk. The design of new prognostic tools should focus on features of respiratory compromise rather than circulatory collapse. We provide a baseline set of variables which are relevant to COVID-19 outcomes and may be used as a basis for developing a bespoke COVID-19 prognostication tool.
Keywords: pneumonia; respiratory infection; viral infection.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- International Severe Acute Respiratory and Emerging Infections Consortium COVID-19 report; 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous