

Comparative efficacy, tolerability and safety of dolutegravir and efavirenz 400mg among antiretroviral therapies for first-line HIV treatment: A systematic literature review and network meta-analysis
- PMID: 33294805
- PMCID: PMC7700905
- DOI: 10.1016/j.eclinm.2020.100573
Comparative efficacy, tolerability and safety of dolutegravir and efavirenz 400mg among antiretroviral therapies for first-line HIV treatment: A systematic literature review and network meta-analysis
Abstract
Background: To inform World Health Organization (WHO) global guidelines, we updated and expanded the evidence base to assess the comparative efficacy, tolerability, and safety of first-line antiretroviral therapy (ART) regimens.
Methods: We searched Embase, Medline and CENTRAL on 28 February 2020 to update the systematic literature review of clinical trials comparing recommended first-line ART that informed previous WHO guidelines. Outcomes included viral suppression, change in CD4 cell counts, mortality, serious and overall adverse events (AEs), discontinuation, discontinuations due to AEs (DAEs); and new outcomes: drug-resistance, neuropsychiatric AEs, early viral suppression, weight gain and birth outcomes. Comparative effects were assessed through network meta-analyses and certainty in the evidence was assessed using the GRADE framework.
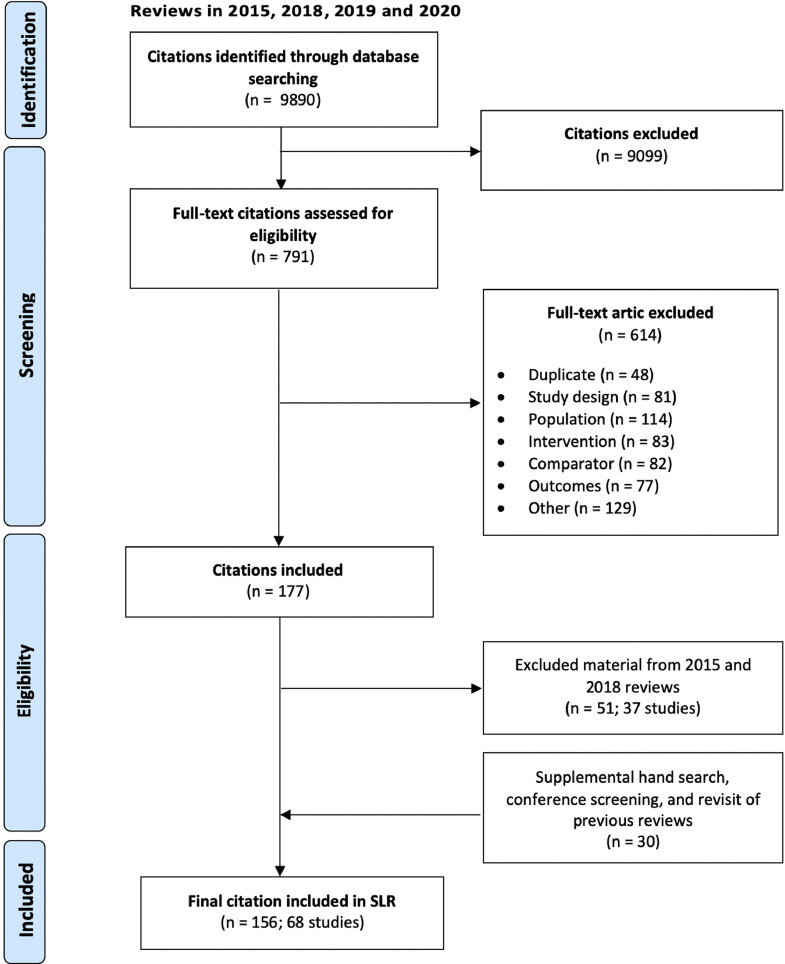
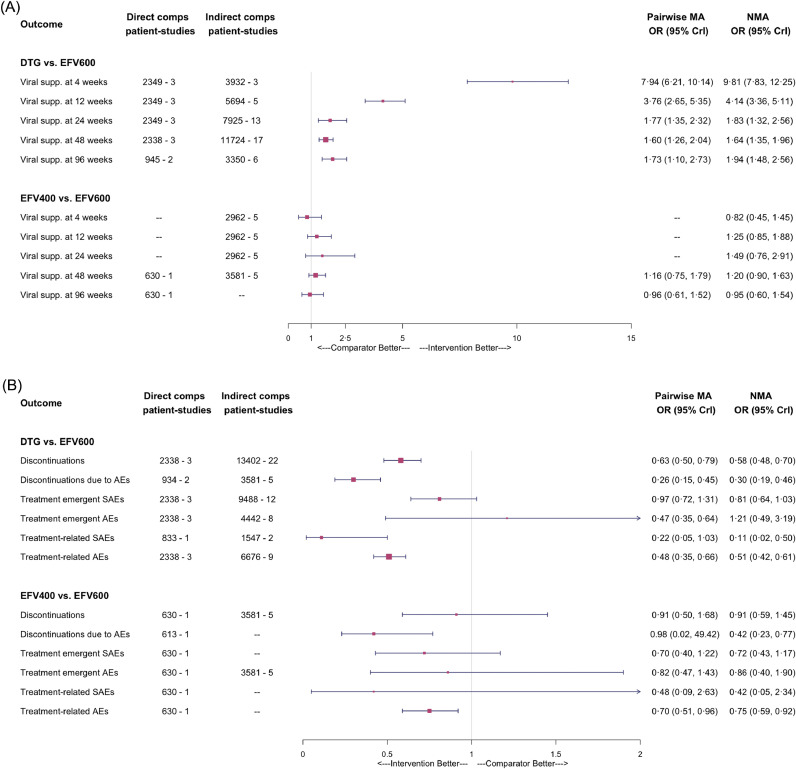
Findings: We identified 156 publications pertaining to 68 trials for the primary population. Relative to efavirenz, dolutegravir had improved odds of viral suppression across all time points (odds ratio [OR]: 1·94; 95% credible interval [CrI]: 1·48-2·56 at 96 weeks); was protective of drug-resistance (OR: 0·13; 95%CrI: 0·04-0·48); and led to fewer discontinuations (OR: 0·58; 95%CrI: 0·48-0·70). Evidence supported dolutegravir use among TB-HIV co-infected persons and pregnant women. Adverse birth outcomes were observed in 33.2% of dolutegravir-managed pregnancies and 35.0% of efavirenz-managed pregnancies. Low-dose efavirenz had comparable efficacy and safety to standard-dose efavirenz, but led to fewer DAEs (OR: 0·70; 95%CrI: 0·50-0·92).
Interpretation: The evidence supports choosing dolutegravir in combination with lamivudine/emtricitabine and tenofovir disoproxil fumarate as the preferred first-line regimen and low-dose efavirenz-based regimens as an alternative. Dolutegravir can be considered to be effective, safe and tolerable.
Funding: WHO.
Keywords: Antiretroviral therapy; First-line; HIV; Network meta-analysis.
© 2020 Published by Elsevier Ltd.
Conflict of interest statement
Dr. Karim reports grants from Michael Smith Foundation for Health Research, grants from Natural Sciences and Engineering Research Council, grants from BC SUPPORT Unit, grants from Canadian Institutes of Health Research, personal fees from Biogen Inc., outside the submitted work. Dr. Alexandra reports grants from Unrestriceted Educational Grant (for the Unit) by MSD and Gilead Sciences, grants from Financial support by Gilead Sciences, AbbVie, MSD, ViiV Healthcare and Janssen Cilag for the day hospital, outside the submitted work. All other authors have nothing to declare.
Figures


References
-
- World Health Organization . 2016. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection recommendations for a public health approach - Second edition. Geneva, Switzerland. - PubMed
-
- Kanters S., Vitoria M., Doherty M. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and network meta-analysis. Lancet HIV. 2016;3(11) e510–e20. - PubMed
-
- Mills E.J., Bakanda C., Birungi J. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med. 2011;155(4):209–216. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
