

Risk factors for indicators of opioid-related harms amongst people living with chronic non-cancer pain: Findings from a 5-year prospective cohort study
- PMID: 33294810
- PMCID: PMC7700907
- DOI: 10.1016/j.eclinm.2020.100592
Risk factors for indicators of opioid-related harms amongst people living with chronic non-cancer pain: Findings from a 5-year prospective cohort study
Abstract
Background: The literature suggests patient characteristics and higher opioid doses and long-term duration are associated with problematic opioid behaviours but no one study has examined the role of all these factors simultaneously in a long-term prospective cohort study.
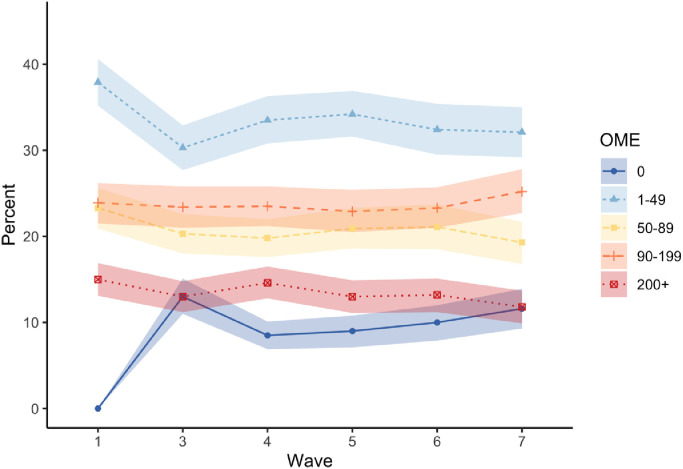
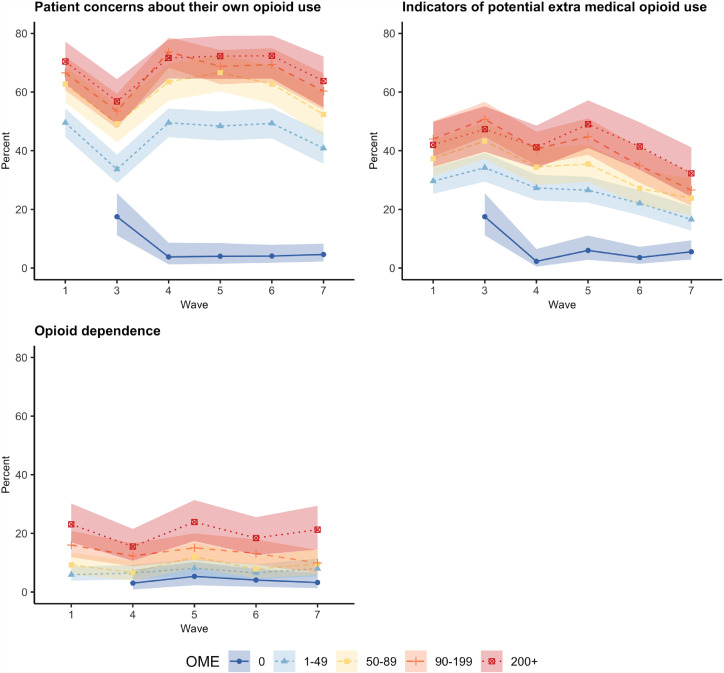
Methods: Five-year, community-based, prospective cohort of people prescribed opioids for chronic non-cancer pain (CNCP). Logistic mixed effect models with multiple imputation were used to address missing data. Oral morphine equivalent (OME) mg per day was categorised as: 0 mg OME/day, 1-49 mg OME/day (reference), 50-89 mg OME/day, 90-199 mg OME/day and 200mg+ OME/day. Patient risk factors included: age, gender, substance use, mental health history and pain-related factors. Main outcomes included: Prescribed Opioids Difficulties Scale (PODS), Opioid-Related Behaviours In Treatment (ORBIT) scale, and ICD-10 opioid dependence. Multiple confounders for problematic opioid behaviours were assessed.
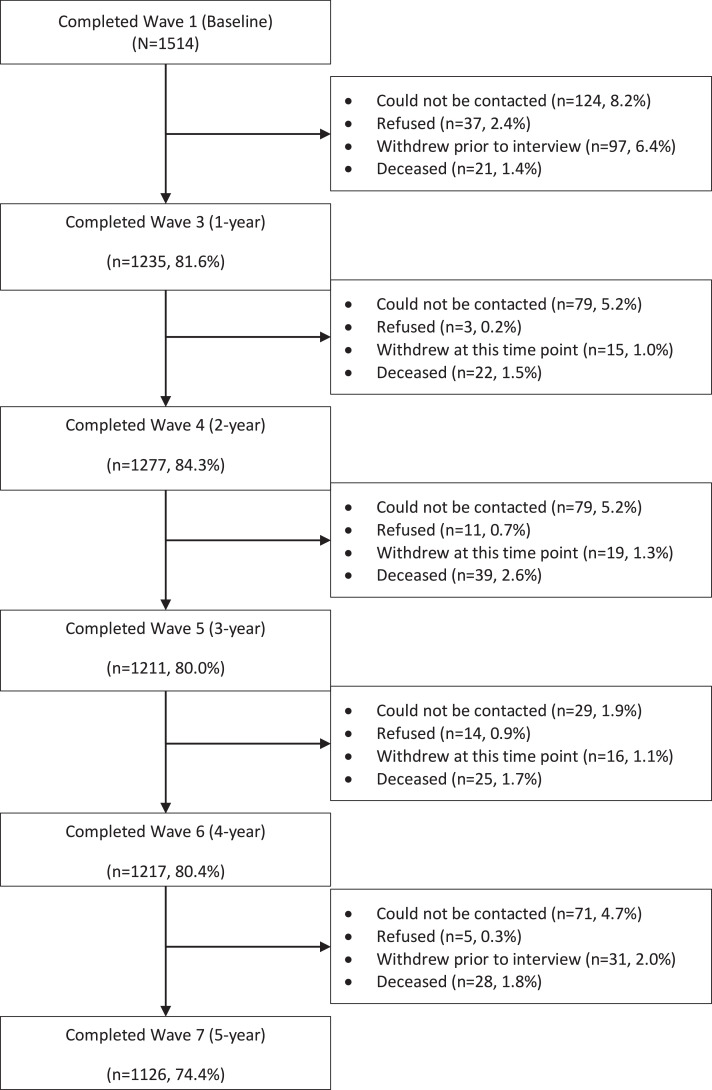
Findings: Of 1,514 participants 44.4% were male (95%CI 41.9-46.9) and their mean age was 58 years (IQR 48-67). Participants had a mean duration of pain of 10 years (IQR 4.5-20.0) and had been taking strong opioids for a median of four years (IQR 1.0-10.0). At baseline, median OME/day was 73 (IQR 35-148). At 5-years, 85% were still taking strong opioids. PODS moderate-high scores reduced from 59.9% (95%CI 58.8-61.0) at baseline to 51.5% (95%CI 50.0-53.0) at 5-years. Around 9% met criteria for ICD-10 opioid dependence at each wave. In adjusted mixed effect models, the risk factors most consistently associated with problematic opioid use were: younger age, substance dependence, mental health histories and higher opioid doses.
Interpretation: Both patient risk factors and opioid dose are associated with problematic opioid use behaviours.
Keywords: Chronic non-cancer pain; Cohort; Dependence; Extra medical use; Pharmaceutical opioid.
© 2020 The Authors.
Conflict of interest statement
GC, LD, MF, RB, MC and SN report grants for the conduct of this study from the National Health and Medical Research Centre (NHMRC). The funder had no input into the design, conduct, data collection, analyses or publication of study findings In the past 36 months some authors have received investigator-driven untied educational grants for unrelated work from Indivior (LD, BL, MF, SN), Mundipharma (MF, RB, NL), Seqirus (LD, MF, BL, SN) and Camurus AB (NL). No company had input into the design, conduct, data collection, analyses or publication of study findings. All other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Pharmaceutical Opioid Use and Dependence among People Living with Chronic Pain: Associations Observed within the Pain and Opioids in Treatment (POINT) Cohort.Pain Med. 2015 Sep;16(9):1745-58. doi: 10.1111/pme.12773. Epub 2015 May 22. Pain Med. 2015. PMID: 26011277
-
Self-reported challenges obtaining ongoing prescription opioids among Australians with chronic non-cancer pain.Int J Drug Policy. 2022 Jul;105:103708. doi: 10.1016/j.drugpo.2022.103708. Epub 2022 May 8. Int J Drug Policy. 2022. PMID: 35544972
-
Agreement between definitions of pharmaceutical opioid use disorders and dependence in people taking opioids for chronic non-cancer pain (POINT): a cohort study.Lancet Psychiatry. 2015 Apr;2(4):314-22. doi: 10.1016/S2215-0366(15)00005-X. Epub 2015 Mar 31. Lancet Psychiatry. 2015. PMID: 26360084
-
Prescribed Dose of Opioids and Overdose: A Systematic Review and Meta-Analysis of Unintentional Prescription Opioid Overdose.CNS Drugs. 2018 Feb;32(2):101-116. doi: 10.1007/s40263-018-0499-3. CNS Drugs. 2018. PMID: 29498021
-
The Effectiveness and Risks of Long-Term Opioid Treatment of Chronic Pain.Evid Rep Technol Assess (Full Rep). 2014 Sep;(218):1-219. doi: 10.23970/AHRQEPCERTA218. Evid Rep Technol Assess (Full Rep). 2014. PMID: 30313000 Review.
Cited by
-
Cross-sectional study of the prevalence of prescription opioids misuse in French patients with chronic non-cancer pain: An update with the French version of the POMI scale.Front Pharmacol. 2022 Sep 5;13:947006. doi: 10.3389/fphar.2022.947006. eCollection 2022. Front Pharmacol. 2022. PMID: 36133827 Free PMC article.
-
U-PAIN cohort study among patients with chronic pain in specialised pain care: a feasibility study.BMJ Open. 2022 Dec 14;12(12):e062265. doi: 10.1136/bmjopen-2022-062265. BMJ Open. 2022. PMID: 36517106 Free PMC article.
-
Mind-body approaches for reducing the need for post-operative opioids: Evidence and opportunities.J Clin Anesth Intensive Care. 2022;3(1):1-5. J Clin Anesth Intensive Care. 2022. PMID: 36590137 Free PMC article. No abstract available.
-
Difficulties with prescribed opioids: a cross-sectional survey of primary care patients in England, United Kingdom.Pain Rep. 2025 Feb 25;10(2):e1246. doi: 10.1097/PR9.0000000000001246. eCollection 2025 Apr. Pain Rep. 2025. PMID: 40012559 Free PMC article.
-
Identifying Prescription-Opioid-Related Risks Using Prescription Drug Monitoring Programs' Algorithms and Clinical Screening Tools.Pharmacy (Basel). 2023 Oct 13;11(5):164. doi: 10.3390/pharmacy11050164. Pharmacy (Basel). 2023. PMID: 37888509 Free PMC article.
References
-
- Kolodny A., Courtwright D.T., Hwang C.S. The prescription opioid and heroin crisis: a public health approach to an epidemic of addiction. Annu Rev Public Health. 2015;36:559–574. - PubMed
-
- Curtis H.J., Croker R., Walker A.J., Richards G.C., Quinlan J., Goldacre B. Opioid prescribing trends and geographical variation in England, 1998–2018: a retrospective database study. Lancet Psychiatry. 2019;6(2):140–150. - PubMed
-
- Chou R., Turner J.A., Devine E.B. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a national institutes of health pathways to prevention workshop. Ann Intern Med. 2015;162(4):276–286. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
