

Immunogenicity of pneumococcal vaccination in HIV infected individuals: A systematic review and meta-analysis
- PMID: 33294820
- PMCID: PMC7695973
- DOI: 10.1016/j.eclinm.2020.100576
Immunogenicity of pneumococcal vaccination in HIV infected individuals: A systematic review and meta-analysis
Abstract
Background: The objective of this systematic review and meta-analysis was to summarise the literature regarding the immunogenicity of pneumococcal conjugate vaccines (PCV) and pneumococcal polysaccharide vaccines (PPSV) in adult people living with HIV (PLWH) in the era of advanced combination antiretroviral therapy (cART).
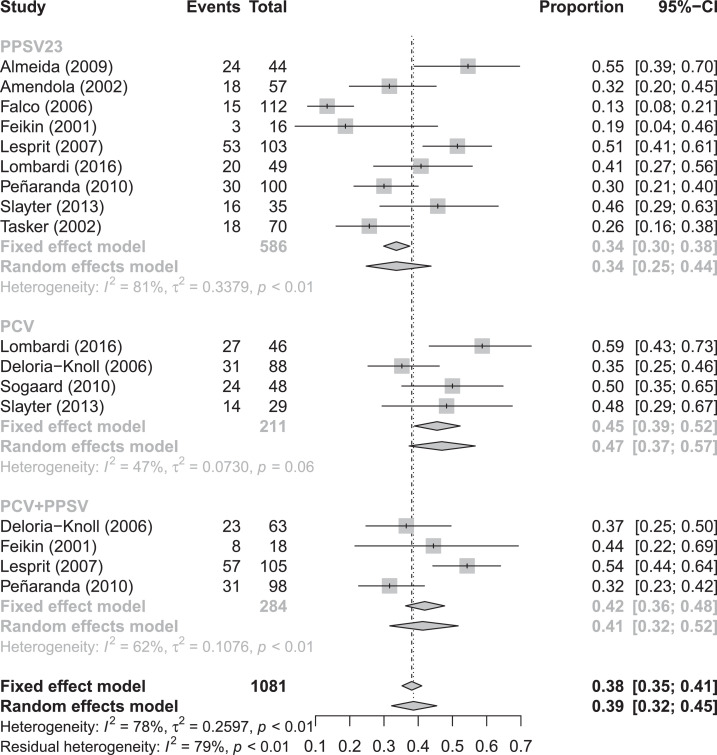
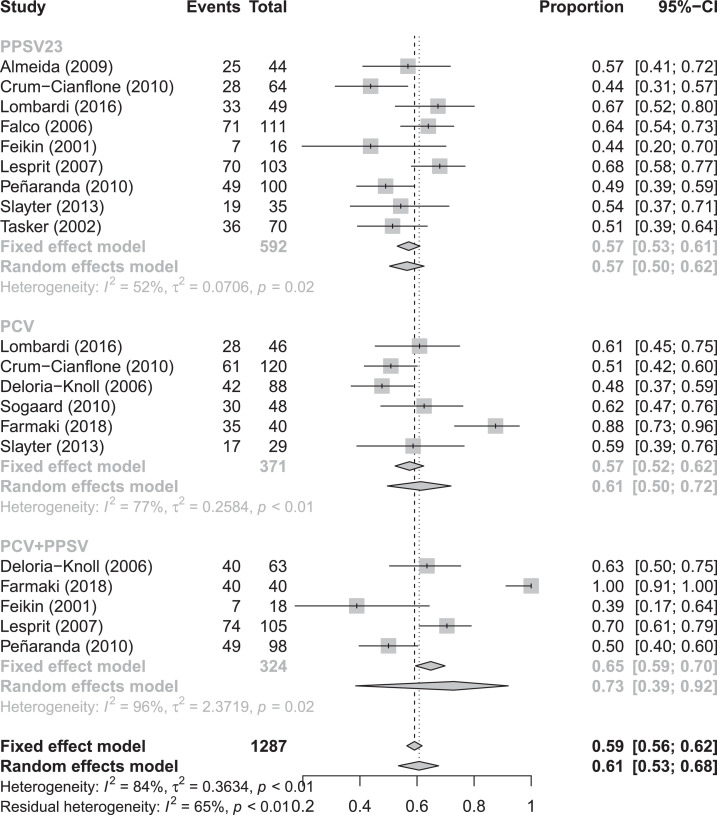
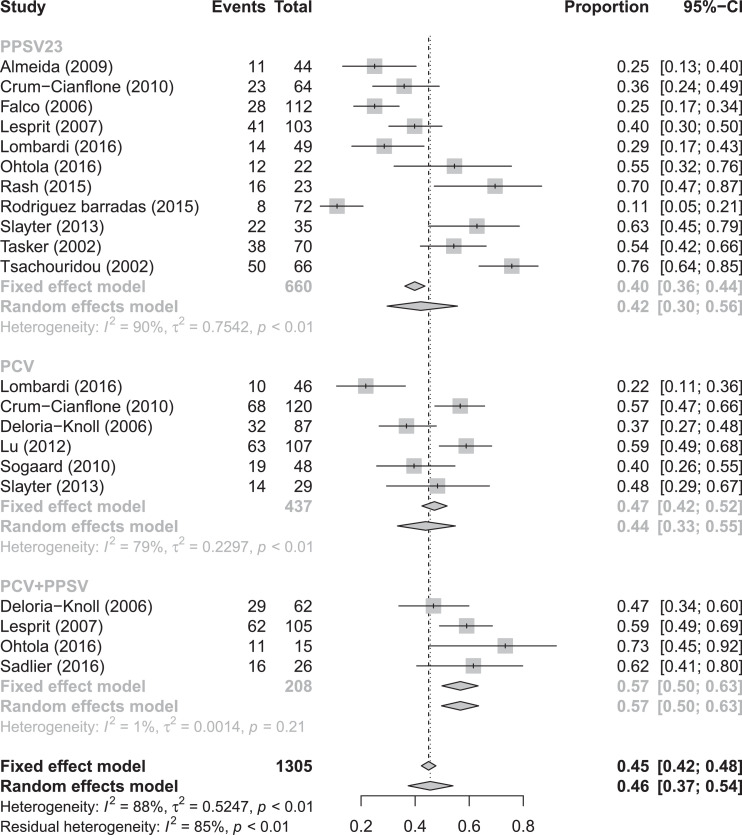
Methods: The systematic review protocol was published online (PROSPERO ID: CRD 42020153137). We searched Medline (Ovid), EMBASE (Ovid), and the Global Health Library for publications from 2000 to June 11, 2020. We included all studies in adult PLWH that reported vaccine immunogenicity outcomes. The primary outcome was seroconversion rate (SCR) after PCV, PPSV and PCV/PPSV combined. For random-effects meta-analysis, we included studies defining SCR as a ≥ 2-fold increase in IgG from baseline, and reporting SCR for serotypes 6B, 14, or overall SCR, 1-3 months after vaccination.
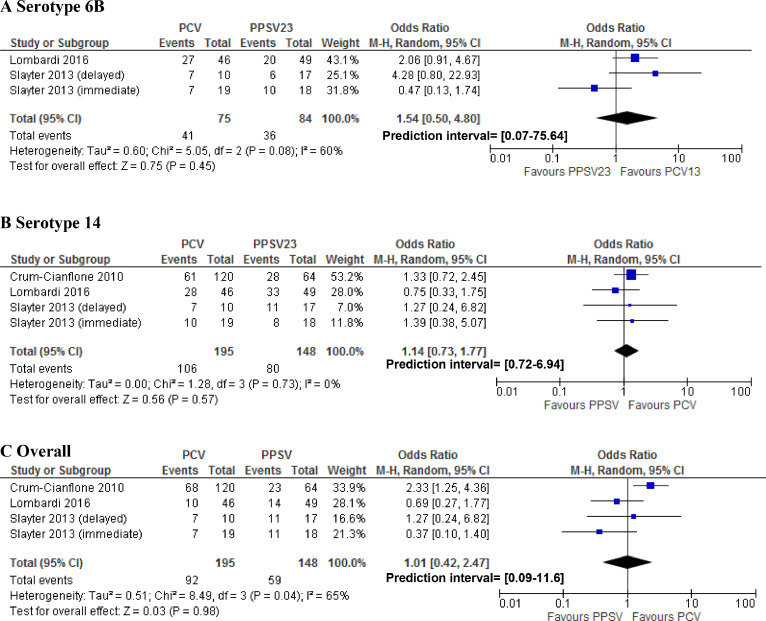
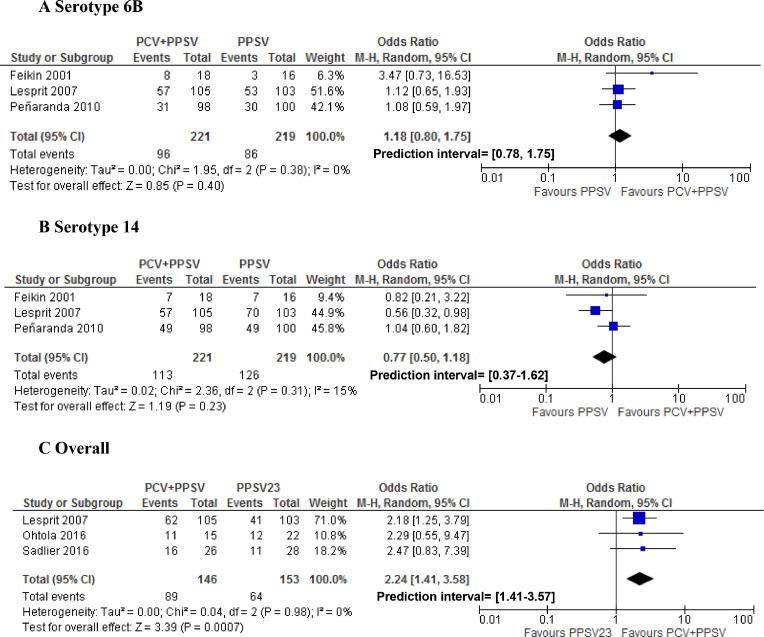
Findings: Our search identified 1597 unique studies, of which 115 were eligible for full-text assessment. Of these, 39 met the inclusion criteria (11 RCTs; 28 cohort studies). A high degree of heterogeneity was observed. Nineteen studies were included in the meta-analysis. Pooled overall SCRs were 42% (95% CI 30-56%), 44% (95% CI 33-55%) and 57% (95% CI 50-63%) for PLWH who received PPSV, PCV or a combination of PCV/PPSV, respectively. Compared to PPSV alone, a combination of PCV/PPSV yielded higher SCRs (OR 2.24 95% CI 1.41- 3.58), whereas we did not observe a significant difference in SCR between PCV and PPSV23 alone. There were no statistically significant differences in geometric mean post-vaccination antibody concentrations between vaccination schedules. Vaccination at higher CD4 cell counts improved immunogenicity in 8/21 studies, especially when PCV was administered. No studies assessed the long-term immunogenicity of PCV followed by PPSV23. Quality of evidence ranged from poor (n = 19) to good quality (n = 7). A limited number of pneumococcal serotypes was assessed in the majority of studies.
Interpretation: We show that the recommended immunisation schedule consisting of a combination of PCV13/PPSV23, is immunogenic in PLWH in the era of advanced cART. However, the durability of this vaccination schedule remains unknown and must be addressed in future research. Vaccination with PCV should be delayed until immunological recovery (CD4>200) in recently diagnosed PLWH for optimal immunogenicity. The evidence gathered here supports wide implementation of the combination of PCV/PPSV23 for all PLWH. We recommend reassessment of this strategy once higher-valent PCVs become available.
Funding: HMGG is funded by a public research grant of ZonMw (project number 522004005).
Keywords: 13valent; 23-valent; Conjugate vaccine; HIV; Invasive pneumococcal disease; Pneumococcal; Pneumonia; Polysaccharide vaccine; Vaccination.
© 2020 The Authors.
Conflict of interest statement
H.M. Garcia Garrido reports being funded by a public research grant from Zon MW, outside the submitted work. None of the other authors report a conflict of interest. All authors attest they meet the ICMJE criteria for authorship.
Figures

References
-
- Garcia Garrido H.M., Mak A.M.R., Wit F. Incidence and risk factors for invasive pneumococcal disease and community-acquired pneumonia in human immunodeficiency virus-infected individuals in a high-income setting. Clin Infect Dis. 2019 doi: 10.1093/cid/ciz728. epub ahead of print. - DOI - PMC - PubMed
-
- van Aalst M., Lotsch F., Spijker R. Incidence of invasive pneumococcal disease in immunocompromised patients: a systematic review and meta-analysis. Travel Med Infect Dis. 2018;24:89–100. - PubMed
-
- Farmaki P.F., Chini M.C., Mangafas N.M. Immunogenicity and Immunological Memory Induced by the 13-Valent Pneumococcal Conjugate Followed by the 23-Valent Polysaccharide Vaccine in HIV-Infected Adults. J Infect Dis. 2018;218(1):26–34. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
