

Left atrial function and maximal exercise capacity in heart failure with preserved and mid-range ejection fraction
- PMID: 33295106
- PMCID: PMC7835603
- DOI: 10.1002/ehf2.13143
Left atrial function and maximal exercise capacity in heart failure with preserved and mid-range ejection fraction
Abstract
Aims: Exercise intolerance is the leading manifestation of heart failure with preserved or mid-range ejection fraction (HFpEF or HFmrEF), and left atrial (LA) function might contribute to modulating left ventricular filling and pulmonary venous pressures. We aim to assess the association between LA function and maximal exercise capacity in patients with HFpEF or HFmrEF.
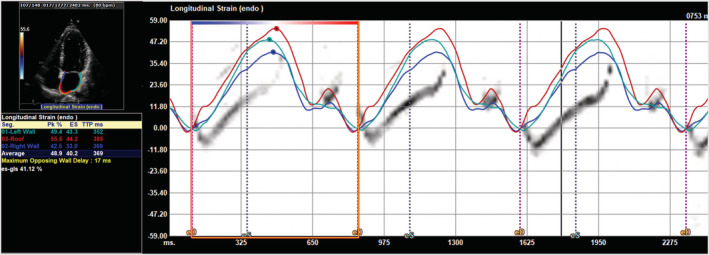
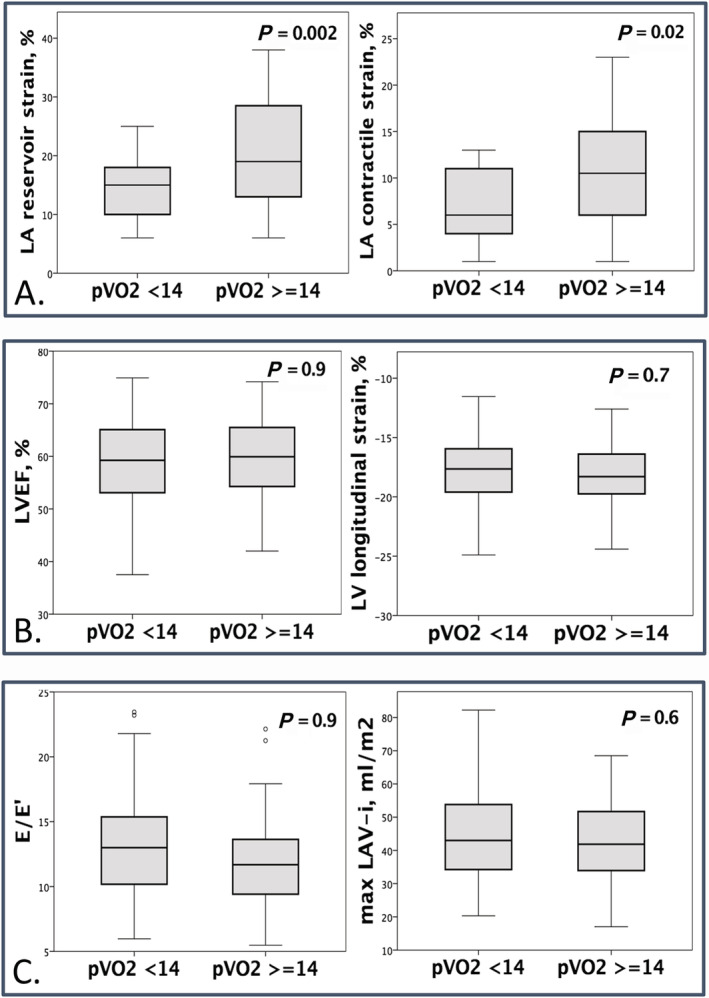
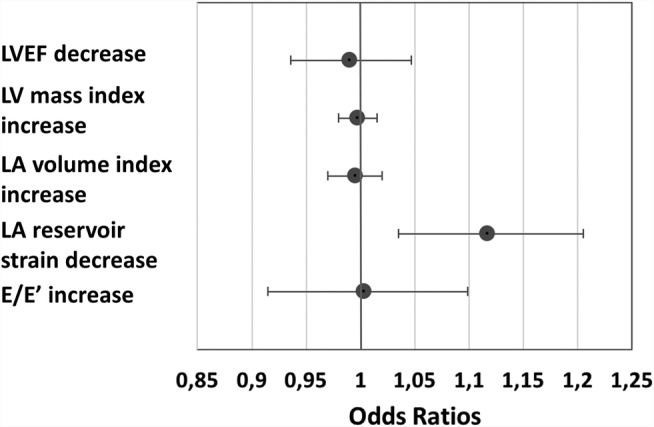
Methods and results: Sixty-five patients, prospectively enrolled in the German HFpEF Registry, were analysed. Inclusion criteria were New York Heart Association functional class ≥ II, left ventricular ejection fraction > 40%, structural heart disease or diastolic dysfunction, and elevated levels of N terminal pro brain natriuretic peptide (NT-proBNP). LA function was evaluated through speckle-tracking echocardiography by central reading in the Charité Academic Echocardiography core lab. All patients underwent maximal cardiopulmonary exercise test and were classified according to a peak VO2 cut-off of prognostic value (14 mL/kg/min). NT-pro-BNP was measured. Twenty-nine patients (45%) reached a peak VO2 < 14 mL/kg/min (mean value 12.4 ± 1.5) and 36 patients (55%) peak VO2 ≥ 14 mL/kg/min (mean value 19.4 ± 3.9). There was no significant difference in left ventricular ejection fraction (60 ± 9 vs. 59 ± 8%), left ventricular mass (109 ± 23 vs. 112 ± 32 g/m2 ), LA volume index (45 ± 17 vs. 47 ± 22 mL/m2 ), or E/e´ (13.1 ± 4.7 vs. 13.0 ± 6.0) between these groups. In contrast, all LA strain measures were impaired in patients with lower peak VO2 (reservoir strain 14 ± 5 vs. 21 ± 9%, P = 0.002; conduit strain 9 ± 2 vs. 13 ± 4%, P = 0.001; contractile strain 7 ± 4 vs. 11 ± 6%, P = 0.02; reported lower limits of normality for LA reservoir, conduit and contractile strains: 26.1%, 12.0%, and 7.7%). In linear regression analysis, lower values of LA reservoir strain were associated with impaired peak VO2 after adjustment for age, sex, body mass index, heart rhythm (sinus/AFib), and log-NTproBNP [β 0.29, 95% confidence interval (CI) 0.02-0.30, P = 0.02], with an odds ratio 1.22 (95% CI 1.05-1.42, P = 0.01) for peak VO2 < 14 mL/kg/min for LA reservoir strain decrease after adjustment for these five covariates. Adding left ventricular ejection fraction, it did not influence the results. On the other hand, the addition of LA strain to the adjustment parameters alone described above provided a significant increase of the predictive value for lower peak VO2 values (R2 0.50 vs. 0.45, P = 0.02). With receiver operating characteristic curve analysis, we identified LA reservoir strain < 22% to have 93% sensitivity and 49% specificity in predicting peak VO2 < 14 mL/kg/min. Using this cut-off, LA reservoir strain < 22% was associated with peak VO2 < 14 mL/kg/min in logistic regression analysis after comprehensive adjustment for age, sex, body mass index, heart rhythm, and log-NTproBNP [odds ratio 95% CI 10.4 (1.4-74), P = 0.02].
Conclusions: In this HFpEF and HFmrEF cohort, a reduction in LA reservoir strain was a sensible marker of decreased peak exercise capacity. Therefore, LA reservoir strain might be of clinical value in predicting exercise capacity in patients with HFpEF or HFmrEF.
Keywords: Cardiopulmonary exercise test; Heart failure; Left atrial strain; Mid-range ejection fraction; Preserved ejection fraction.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Redfield MM. Heart failure with preserved ejection fraction. N Engl J Med 2017; 376: 897. - PubMed
-
- Nauta JF, Hummel YM, van Melle JP, van der Meer P, Lam CSP, Ponikowski P, Voors AA. What have we learned about heart failure with mid‐range ejection fraction one year after its introduction? Eur J Heart Fail 2017; 19: 1569–1573. - PubMed
-
- Edelmann F, Gelbrichb G, Duvinage A, Stahrenberg R, Behrens A, Prettin C. Differential interaction of clinical characteristics with key functional parameters in heart failure with preserved ejection fraction—results of the Aldo‐DHF trial. Int J Cardiol 2013; 169: 408–417. - PubMed
-
- Nauta JF, Hummel YM, van der Meer P, Lam CSP, Voors AA, van Melle JP. Correlation with invasive left ventricular filling pressures and prognostic relevance of the echocardiographic diastolic parameters used in the 2016 ESC heart failure guidelines and in the 2016 ASE/EACVI recommendations: a systematic review in patients with heart failure with preserved ejection fraction. Eur J Heart Fail 2018; 20: 1303–1311. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
