

The maturation changes of sleep-related respiratory abnormalities in infants with laryngomalacia
- PMID: 33295276
- PMCID: PMC8020689
- DOI: 10.5664/jcsm.9046
The maturation changes of sleep-related respiratory abnormalities in infants with laryngomalacia
Abstract
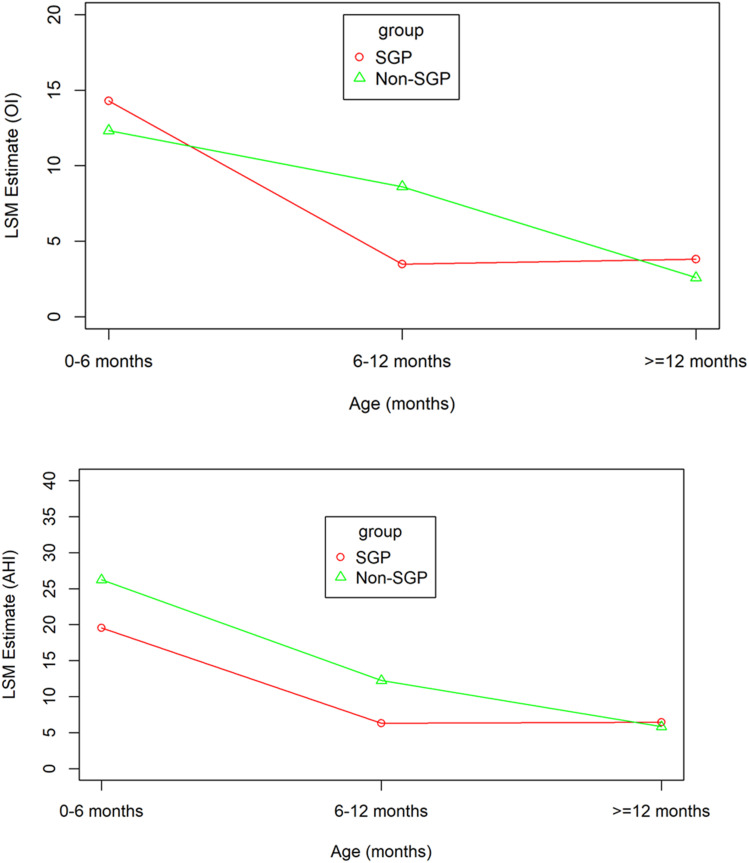
Study objectives: Obstructive sleep apnea (OSA) and central sleep apnea (CSA) are common in infants with laryngomalacia. The purpose of this study was to evaluate developmental changes in sleep-related breathing disorders over time in infants with laryngomalacia and understand the effect of supraglottoplasty (SGP) and nonsurgical treatment.
Methods: This is a retrospective review of infants with laryngomalacia who had at least 2 diagnostic polysomnography studies performed from January 2000 and May 2015. We included infants who had either OSA or CSA. Comparison of sleep and respiratory parameters by age group (0-6, 6-12, and >12 months old) was performed in both SGP and non-SGP groups using a mixed-effect regression model. A log-normal mixed model was used to explore the changes in sleep and respiratory parameters with age. The time to resolution of CSA and OSA was analyzed using nonparametric survival analysis.
Results: A total of 102 infants were included; 57 had only OSA and 45 had both CSA and OSA. There were significant decreases in apnea-hypopnea index, obstructive index, central apnea index, and arousal index with increasing age in both SGP and non-SGP groups. The mean age at resolution of CSA (central apnea index < 5) was 7.60 months old for SGP and 12.57 months old for non-SGP (P < .05). There were no significant differences in the mean age at resolution of OSA (obstructive index < 1; 35.18 [SGP] vs 41.55 months [non-SGP]; P = .60) between SGP and non-SGP groups. Infants with neurologic disease, congenital anomalies, or genetic syndromes required significantly more time to resolve OSA (28.12 [normal] vs 53.13 [neurological] vs 59.53 months [congenital anomalies and genetic]; P < .01).
Conclusions: Both OSA and CSA improve in infants with laryngomalacia with increasing age regardless of SGP. The mechanism underlying these changes may involve airway growth and maturation of respiratory control. Time to resolution of OSA is affected by the presence of neurologic diseases, congenital anomalies, and genetic syndromes. Further studies are needed to confirm these findings and to evaluate long-term outcomes in this population.
Keywords: central sleep apnea; developmental changes of sleep apnea; laryngomalacia; obstructive sleep apnea.
© 2021 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have seen and approved the manuscript. The study was funded by the Cincinnati Children’s Research Foundation. Part of this research was presented as an abstract at the International conference of the American Thoracic Society 2017. The authors report no conflicts of interest.
Figures



Comment in
-
Laryngomalacia in infancy improves with increasing age irrespective of treatment.J Clin Sleep Med. 2021 Apr 1;17(4):619-620. doi: 10.5664/jcsm.9128. J Clin Sleep Med. 2021. PMID: 33551020 Free PMC article.
Similar articles
-
Supraglottoplasty for laryngomalacia with obstructive sleep apnea.Laryngoscope. 2008 Oct;118(10):1873-7. doi: 10.1097/MLG.0b013e31817e7441. Laryngoscope. 2008. PMID: 18641529
-
Polysomnographic parameters and clinical risk factors predicting postoperative respiratory complications in children undergoing supraglottoplasty.J Clin Sleep Med. 2024 Jan 1;20(1):9-16. doi: 10.5664/jcsm.10770. J Clin Sleep Med. 2024. PMID: 37584453 Free PMC article.
-
Changes in sleep apnea after supraglottoplasty in infants with laryngomalacia.Int J Pediatr Otorhinolaryngol. 2011 Oct;75(10):1234-9. doi: 10.1016/j.ijporl.2011.06.021. Epub 2011 Aug 3. Int J Pediatr Otorhinolaryngol. 2011. PMID: 21816491
-
Treatment outcomes of supraglottoplasty for pediatric obstructive sleep apnea: A meta-analysis.Int J Pediatr Otorhinolaryngol. 2016 Aug;87:18-27. doi: 10.1016/j.ijporl.2016.05.015. Epub 2016 May 20. Int J Pediatr Otorhinolaryngol. 2016. PMID: 27368437 Review.
-
Objective Outcomes of Supraglottoplasty for Children With Laryngomalacia and Obstructive Sleep Apnea: A Meta-analysis.JAMA Otolaryngol Head Neck Surg. 2016 Jul 1;142(7):665-71. doi: 10.1001/jamaoto.2016.0830. JAMA Otolaryngol Head Neck Surg. 2016. PMID: 27259063 Review.
Cited by
-
Sleep Studies for Clinical Indications during the First Year of Life: Infants Are Not Small Children.Children (Basel). 2022 Apr 7;9(4):523. doi: 10.3390/children9040523. Children (Basel). 2022. PMID: 35455567 Free PMC article.
-
An update on diagnosis and management of obstructive sleep apnoea in the first 2 years of life.Eur Respir Rev. 2024 Jan 31;33(171):230121. doi: 10.1183/16000617.0121-2023. Print 2024 Jan 31. Eur Respir Rev. 2024. PMID: 38296343 Free PMC article. Review.
-
An Analysis of Laryngomalacia and Its Interplay With Obesity and Obstructive Sleep Apnea in Pediatric Inpatients.Cureus. 2023 Sep 15;15(9):e45313. doi: 10.7759/cureus.45313. eCollection 2023 Sep. Cureus. 2023. PMID: 37846256 Free PMC article.
-
Laryngomalacia in infancy improves with increasing age irrespective of treatment.J Clin Sleep Med. 2021 Apr 1;17(4):619-620. doi: 10.5664/jcsm.9128. J Clin Sleep Med. 2021. PMID: 33551020 Free PMC article.
-
Upper airway obstruction during sleep in infants with laryngomalacia is frequently sleep-position-dependent.Pediatr Res. 2025 Feb 13. doi: 10.1038/s41390-025-03919-z. Online ahead of print. Pediatr Res. 2025. PMID: 39948383
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
