

Association of culprit lesion plaque characteristics with flow restoration post-fibrinolysis in ST-segment elevation myocardial infarction: an intravascular ultrasound-virtual histology study
- PMID: 33296051
- PMCID: PMC7726087
- DOI: 10.1186/s43044-020-00121-w
Association of culprit lesion plaque characteristics with flow restoration post-fibrinolysis in ST-segment elevation myocardial infarction: an intravascular ultrasound-virtual histology study
Erratum in
-
Correction to: Association of culprit lesion plaque characteristics with flow restoration post-fibrinolysis in ST-segment elevation myocardial infarction: an intravascular ultrasound-virtual histology study.Egypt Heart J. 2020 Dec 20;72(1):88. doi: 10.1186/s43044-020-00125-6. Egypt Heart J. 2020. PMID: 33341905 Free PMC article. No abstract available.
Abstract
Background: Not every patient achieves normal coronary flow following fibrinolysis in STEMI (ST-segment elevation myocardial infarction). The culprit lesion plaque characteristics play a prominent role in the coronary flow before and during percutaneous coronary intervention. The main purpose was to determine the culprit lesion plaque features by virtual histology-intravascular ultrasound (VH-IVUS) in patients with STEMI following fibrinolysis in relation to baseline coronary angiogram TIMI (thrombolysis in myocardial infarction) flow. Pre-intervention IVUS was undertaken in 61 patients with STEMI after successful fibrinolysis. After the coronary angiogram, they were separated into the TIMI1-2 flow group (n = 31) and TIMI 3 flow group (n = 30). Culprit lesion plaque composition was evaluated by VH-IVUS.
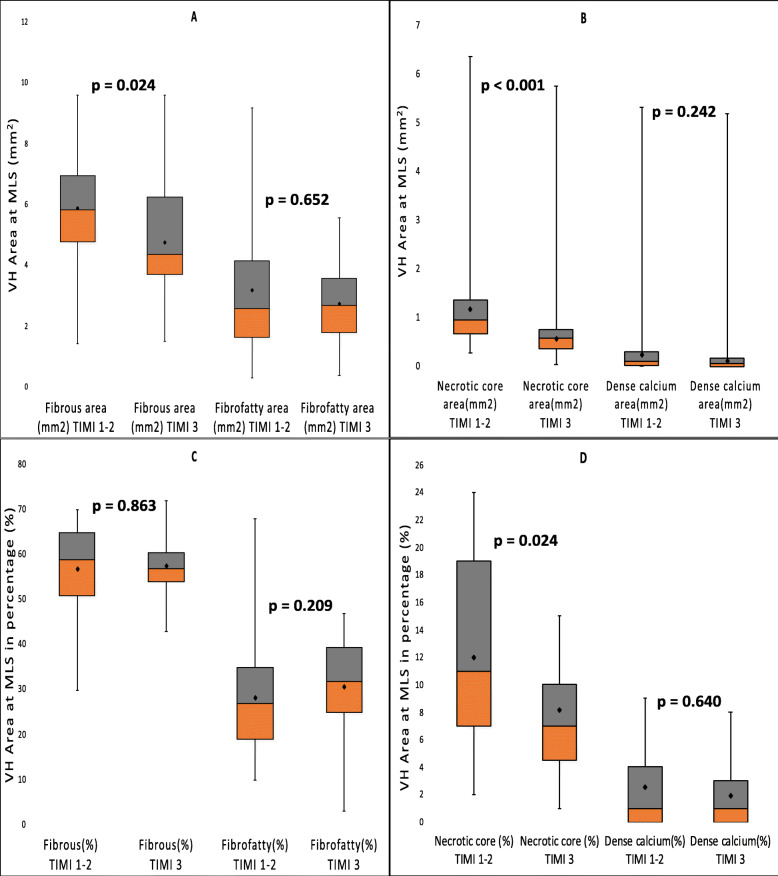
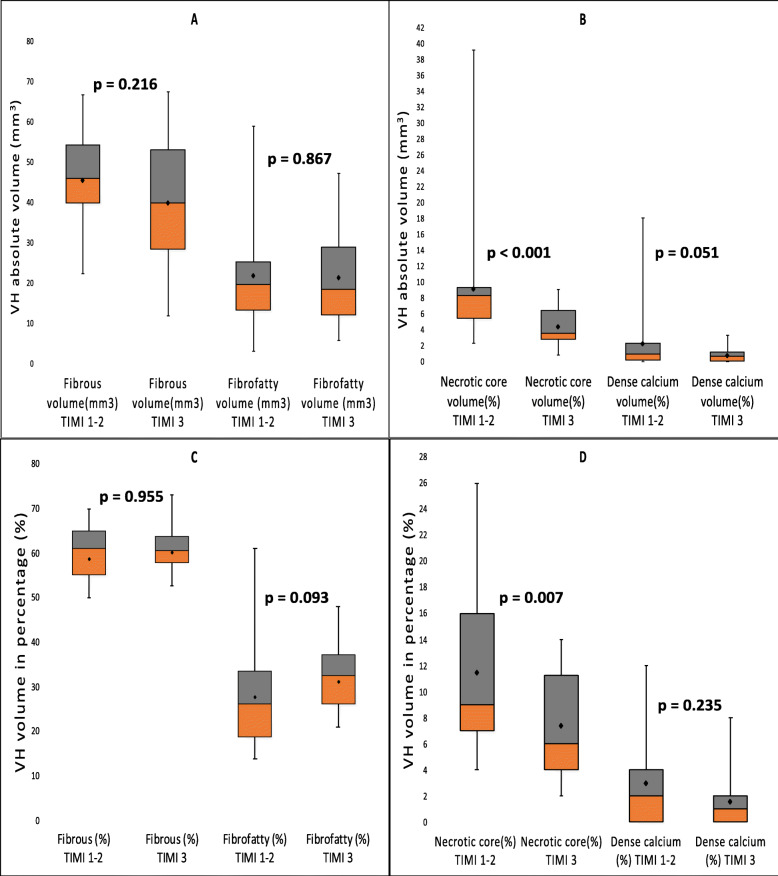
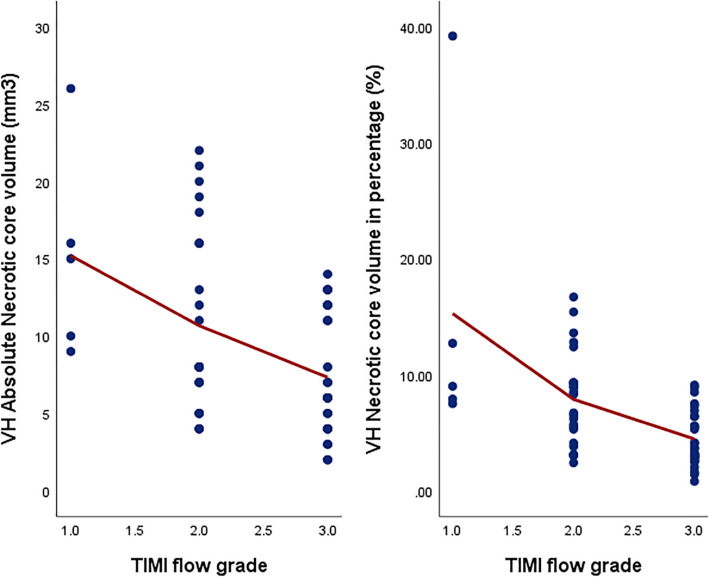
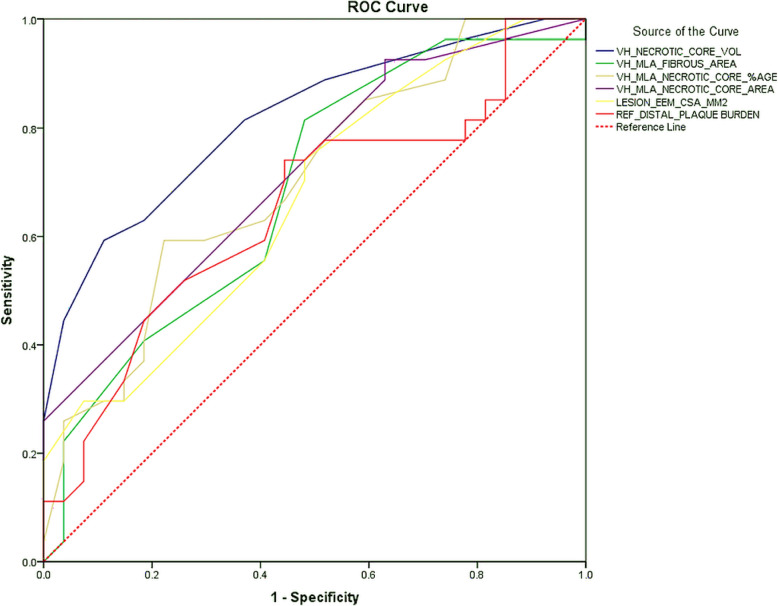
Results: On gray-scale IVUS, the lesion external elastic membrane cross-sectional area (EEM CSA) was significantly higher in the TIMI 1-2 groups as compared to the TIMI 3 group (15.71 ± 3.73 mm2 vs 13.91 ± 2.94 mm2, p = 0.041) with no significant difference in plaque burden (82.42% vs. 81.65%, p = 0.306) and plaque volume (108.3 mm3 vs. 94.3 mm3, p = 0.194). On VH-IVUS, at the minimal luminal area site (MLS), the fibrous area (5.83 mm2 vs. 4.37 mm2, p = 0.024), necrotic core (NC) area (0.95 mm2 vs. 0.59 mm2, p < 0.001), and NC percentage (11% vs. 7.1%, p = 0.024) were higher in the TIMI 1-2 groups in contrast to the TIMI 3 group. The absolute necrotic core (NC) volume (8.3 mm3 vs. 3.65 mm3, p < 0.001) and NC percentage (9.3% vs. 6.0%, p = 0.007) were significantly higher in the TIMI 1-2 groups as compared to the TIMI 3 group. Absolute dense calcium (DC) volume was higher in TIMI 1-2 groups with a trend towards significance (1.0 mm3 vs.0.75 mm3, p = 0.051). In multivariate analysis, absolute NC volume was the only independent predictor of TIMI 1-2 flow (odds ratio = 1.561; 95% CI 1.202-2.026, p = 0.001). Receiver operating characteristic curves showed absolute NC volume has best diagnostic accuracy (AUC = 0.816, p < 0.001) to predict TIMI 1-2 flow with an optimal cutoff value of 4.5 mm3 with sensitivity and specificity of 79% and 61%, respectively.
Conclusions: This study exemplifies that the necrotic core component of the culprit lesion plaque in STEMI is associated with the coronary flow after fibrinolysis. The absolute necrotic core volume is a key determinant of flow restoration post-fibrinolysis and aids in prognostication of less than TIMI 3 flow.
Keywords: Fibrinolysis; Intravascular ultrasound; Necrotic core; ST-segment elevation myocardial infarction; TIMI flow; Virtual histology-intravascular ultrasound.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Impact of culprit plaque volume and composition on myocardial microcirculation following primary angioplasty in patients with ST-segment elevation myocardial infarction: virtual histology intravascular ultrasound analysis.Int J Cardiol. 2013 Aug 10;167(3):1000-5. doi: 10.1016/j.ijcard.2012.03.079. Epub 2012 Apr 4. Int J Cardiol. 2013. PMID: 22481047
-
Impact of plaque burden and composition on coronary slow flow in ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: intravascular ultrasound and virtual histology analysis.Acta Cardiol. 2021 Aug;76(6):650-660. doi: 10.1080/00015385.2020.1767842. Epub 2020 May 26. Acta Cardiol. 2021. PMID: 32452718
-
Association of virtual histology characteristics of the culprit plaque with post-fibrinolysis flow restoration in ST-elevation myocardial infarction.Int J Cardiol. 2014 Jul 1;174(3):678-82. doi: 10.1016/j.ijcard.2014.04.211. Epub 2014 Apr 26. Int J Cardiol. 2014. PMID: 24809918
-
[Impact of inflammatory reaction levels and culprit plaque characteristics on preprocedural thrombolysis in myocardial infarction flow grade in patients with ST-segment elevation myocardial infarction].Zhonghua Xin Xue Guan Bing Za Zhi. 2021 Feb 24;49(2):150-157. doi: 10.3760/cma.j.cn112148-20200531-00452. Zhonghua Xin Xue Guan Bing Za Zhi. 2021. PMID: 33611901 Chinese.
-
Tissue characteristics of culprit lesion and myocardial tissue-level perfusion in non-ST-segment elevation acute coronary syndromes: The EARLY-MYO-ACS study.Int J Cardiol. 2019 Jul 15;287:32-38. doi: 10.1016/j.ijcard.2019.02.010. Epub 2019 Feb 8. Int J Cardiol. 2019. PMID: 30772013
Cited by
-
Correction to: Association of culprit lesion plaque characteristics with flow restoration post-fibrinolysis in ST-segment elevation myocardial infarction: an intravascular ultrasound-virtual histology study.Egypt Heart J. 2020 Dec 20;72(1):88. doi: 10.1186/s43044-020-00125-6. Egypt Heart J. 2020. PMID: 33341905 Free PMC article. No abstract available.
-
Roles of transient receptor potential channel 6 in glucose-induced cardiomyocyte injury.World J Diabetes. 2022 Apr 15;13(4):338-357. doi: 10.4239/wjd.v13.i4.338. World J Diabetes. 2022. PMID: 35582666 Free PMC article.
References
-
- Gersh BJ, Sliwa K, Mayosi BM, Yusuf S. Novel therapeutic concepts: the epidemic of cardiovascular disease in the developing world: global implications. Eur Heart J. 2010;31(6):642–648. - PubMed
-
- Alexander T, Mehta S, Mullasari A, Nallamothu BK. Systems of care for ST-elevation myocardial infarction in India. Heart. 2012;98(1):15–17. - PubMed
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361(9351):13–20. - PubMed
LinkOut - more resources
Full Text Sources