

Coronary 18F-Fluoride Uptake and Progression of Coronary Artery Calcification
- PMID: 33297761
- PMCID: PMC7771641
- DOI: 10.1161/CIRCIMAGING.120.011438
Coronary 18F-Fluoride Uptake and Progression of Coronary Artery Calcification
Abstract
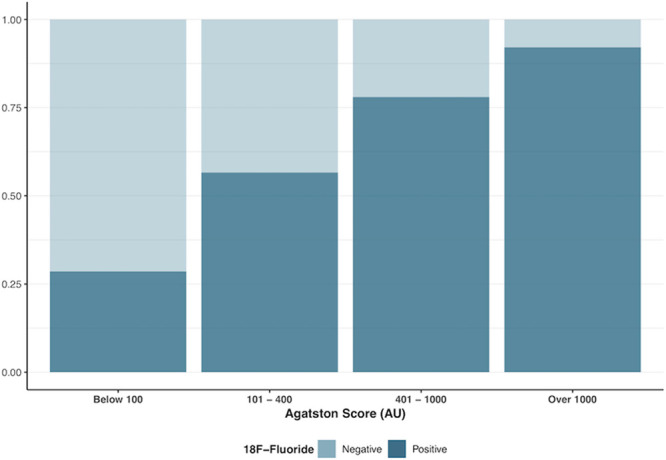
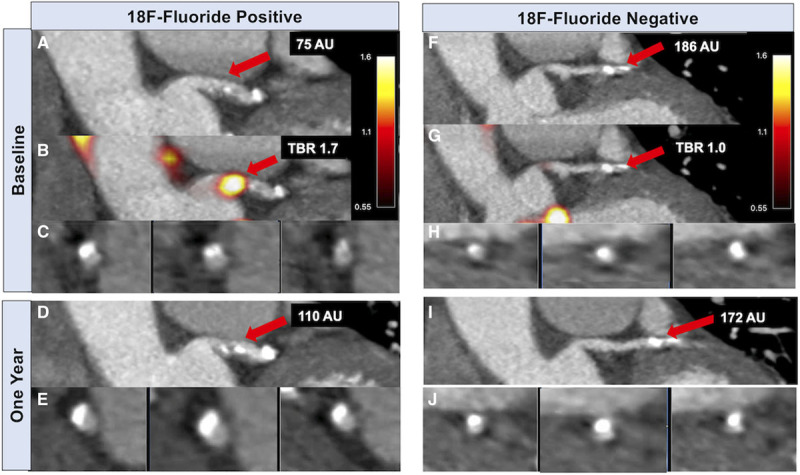
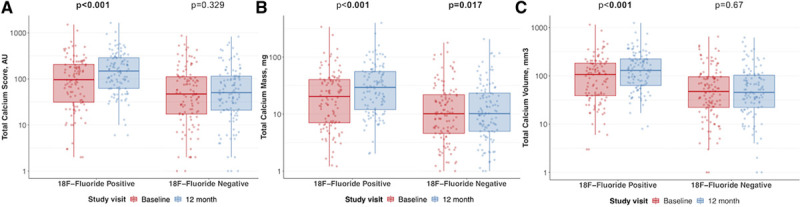
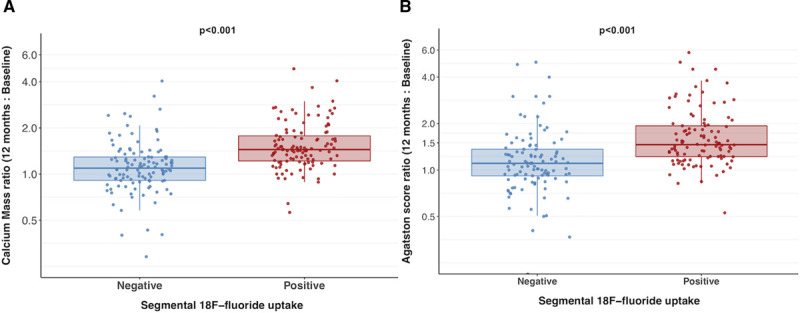
Background Positron emission tomography (PET) using 18F-sodium fluoride (18F-fluoride) to detect microcalcification may provide insight into disease activity in coronary atherosclerosis. This study aimed to investigate the relationship between 18F-fluoride uptake and progression of coronary calcification in patients with clinically stable coronary artery disease. Methods Patients with established multivessel coronary atherosclerosis underwent 18F-fluoride PET-computed tomography angiography and computed tomography calcium scoring, with repeat computed tomography angiography and calcium scoring at one year. Coronary PET uptake was analyzed qualitatively and semiquantitatively in diseased vessels by measuring maximum tissue-to-background ratio. Coronary calcification was quantified by measuring calcium score, mass, and volume. Results In a total of 183 participants (median age 66 years, 80% male), 116 (63%) patients had increased 18F-fluoride uptake in at least one vessel. Individuals with increased 18F-fluoride uptake demonstrated more rapid progression of calcification compared with those without uptake (change in calcium score, 97 [39-166] versus 35 [7-93] AU; P<0.0001). Indeed, the calcium score only increased in coronary segments with 18F-fluoride uptake (from 95 [30-209] to 148 [61-289] AU; P<0.001) and remained unchanged in segments without 18F-fluoride uptake (from 46 [16-113] to 49 [20-115] AU; P=0.329). Baseline coronary 18F-fluoride maximum tissue-to-background ratio correlated with 1-year change in calcium score, calcium volume, and calcium mass (Spearman ρ=0.37, 0.38, and 0.46, respectively; P<0.0001 for all). At the segmental level, baseline 18F-fluoride activity was an independent predictor of calcium score at 12 months (P<0.001). However, at the patient level, this was not independent of age, sex, and baseline calcium score (P=0.50). Conclusions Coronary 18F-fluoride uptake identifies both patients and individual coronary segments with more rapid progression of coronary calcification, providing important insights into disease activity within the coronary circulation. At the individual patient level, total calcium score remains an important marker of disease burden and progression. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT02110303.
Keywords: atherosclerosis; calcium; coronary angiography; positron emission tomography; risk factors.
Conflict of interest statement
Dr Newby has received educational grants, honoraria for consultancy, and lectures from AstraZeneca. The other authors report no conflicts.
Figures
Comment in
-
Correlation of 18F-NaF Activity With Progression of Macrocalcification: Another Step Toward Vulnerable Plaque Detection?Circ Cardiovasc Imaging. 2020 Dec;13(12):e012095. doi: 10.1161/CIRCIMAGING.120.012095. Epub 2020 Dec 10. Circ Cardiovasc Imaging. 2020. PMID: 33297762 No abstract available.
References
-
- Hou ZH, Lu B, Gao Y, Jiang SL, Wang Y, Li W, Budoff MJ. Prognostic value of coronary CT angiography and calcium score for major adverse cardiac events in outpatients. JACC Cardiovasc Imaging. 2012; 5:990–999. doi: 10.1016/j.jcmg.2012.06.006 - PubMed
-
- Arad Y, Spadaro LA, Goodman K, Newstein D, Guerci AD. Prediction of coronary events with electron beam computed tomography. J Am Coll Cardiol. 2000; 36:1253–1260. doi: 10.1016/s0735-1097(00)00872-x - PubMed
-
- Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K, Shea S, Szklo M, Bluemke DA, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008; 358:1336–1345. doi: 10.1056/NEJMoa072100 - PubMed
-
- Budoff MJ, Hokanson JE, Nasir K, Shaw LJ, Kinney GL, Chow D, Demoss D, Nuguri V, Nabavi V, Ratakonda R, et al. Progression of coronary artery calcium predicts all-cause mortality. JACC Cardiovasc Imaging. 2010; 3:1229–1236. doi: 10.1016/j.jcmg.2010.08.018 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- RG/16/10/32375/BHF_/British Heart Foundation/United Kingdom
- FS/18/31/33676/BHF_/British Heart Foundation/United Kingdom
- G0701127/MRC_/Medical Research Council/United Kingdom
- FS/17/79/33226/BHF_/British Heart Foundation/United Kingdom
- PG/19/40/34422/BHF_/British Heart Foundation/United Kingdom
- AA/18/3/34220/BHF_/British Heart Foundation/United Kingdom
- RE/18/5/34216/BHF_/British Heart Foundation/United Kingdom
- R01 HL135557/HL/NHLBI NIH HHS/United States
- WT103782AIA/WT_/Wellcome Trust/United Kingdom
- FS/14/78/31020/BHF_/British Heart Foundation/United Kingdom
- CH/09/002/26360/BHF_/British Heart Foundation/United Kingdom
- FS/17/51/33096/BHF_/British Heart Foundation/United Kingdom
- FS/19/46/34445/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
