

Genetic determinants of clinical phenotype in hypertrophic cardiomyopathy
- PMID: 33297970
- PMCID: PMC7727200
- DOI: 10.1186/s12872-020-01807-4
Genetic determinants of clinical phenotype in hypertrophic cardiomyopathy
Abstract
Background: Hypertrophic cardiomyopathy (HCM) is the most common inherited cardiovascular disease that affects approximately one in 500 people. HCM is a recognized genetic disorder most often caused by mutations involving myosin-binding protein C (MYBPC3) and β-myosin heavy chain (MYH7) which are responsible for approximately three-quarters of the identified mutations.
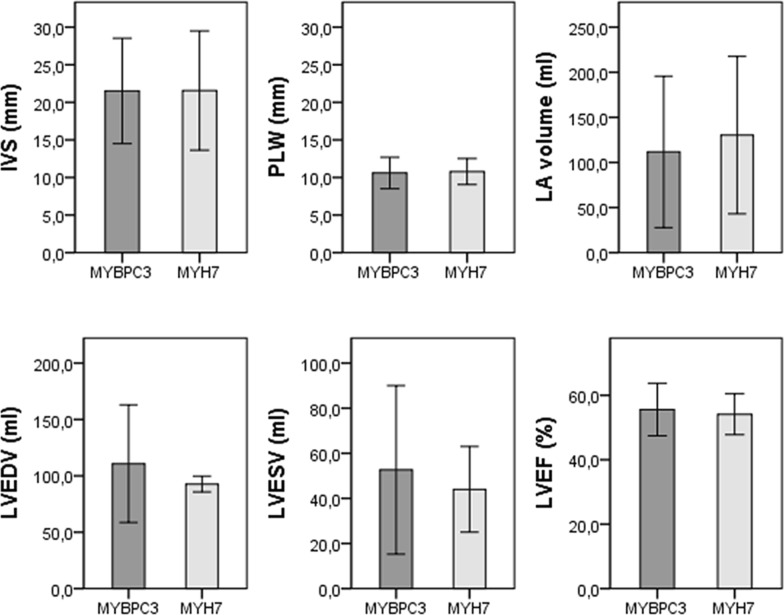
Methods: As a part of the international multidisciplinary SILICOFCM project ( www.silicofcm.eu ) the present study evaluated the association between underlying genetic mutations and clinical phenotype in patients with HCM. Only patients with confirmed single pathogenic mutations in either MYBPC3 or MYH7 genes were included in the study and divided into two groups accordingly. The MYBPC3 group was comprised of 48 patients (76%), while the MYH7 group included 15 patients (24%). Each patient underwent clinical examination and echocardiography.
Results: The most prevalent symptom in patients with MYBPC3 was dyspnea (44%), whereas in patients with MYH7 it was palpitations (33%). The MYBPC3 group had a significantly higher number of patients with a positive family history of HCM (46% vs. 7%; p = 0.014). There was a numerically higher prevalence of atrial fibrillation in the MYH7 group (60% vs. 35%, p = 0.085). Laboratory analyses revealed normal levels of creatinine (85.5 ± 18.3 vs. 81.3 ± 16.4 µmol/l; p = 0.487) and blood urea nitrogen (10.2 ± 15.6 vs. 6.9 ± 3.9 mmol/l; p = 0.472) which were similar in both groups. The systolic anterior motion presence was significantly more frequent in patients carrying MYH7 mutation (33% vs. 10%; p = 0.025), as well as mitral leaflet abnormalities (40% vs. 19%; p = 0.039). Calcifications of mitral annulus were registered only in MYH7 patients (20% vs. 0%; p = 0.001). The difference in diastolic function, i.e. E/e' ratio between the two groups was also noted (MYBPC3 8.8 ± 3.3, MYH7 13.9 ± 6.9, p = 0.079).
Conclusions: Major findings of the present study corroborate the notion that MYH7 gene mutation patients are presented with more pronounced disease severity than those with MYBPC3.
Keywords: HCM; Hereditary cardiac disease; Hypertrophic cardiomyopathy; Left ventricular hypertrophy; MYBPC3; MYH7.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Maron BJ. Clinical course and management of hypertrophic cardiomyopathy. N Engl J Med. 2018;379(20):1977. - PubMed
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(24):2761–2796. doi: 10.1161/CIR.0b013e318223e230. - DOI - PubMed
-
- Authors/Task Force Members. Elliott PM, Anastasakis A, Borger MA, Borggrefe M, Cecchi F, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC) Eur Heart J. 2014;35(39):2733–2779. doi: 10.1093/eurheartj/ehu284. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
