

Impact of the SARS-CoV-2 pandemic on emergency surgery services-a multi-national survey among WSES members
- PMID: 33298131
- PMCID: PMC7724441
- DOI: 10.1186/s13017-020-00341-0
Impact of the SARS-CoV-2 pandemic on emergency surgery services-a multi-national survey among WSES members
Abstract
Background: The SARS-CoV-2 pandemic is a major challenge for health care services worldwide. It's impact on oncologic therapies and elective surgery has been described recently, and the literature provides guidelines regarding appropriate elective patient treatment during the pandemic. However, the impact of SARS-CoV-2 pandemic on emergency surgery services has been poorly investigated up to now.
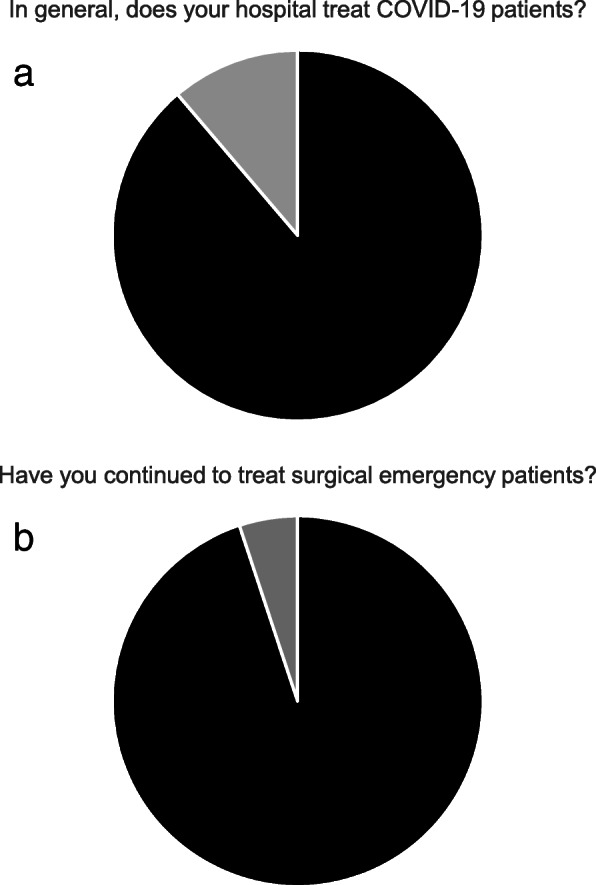
Methods: A 17-item web survey had been distributed to emergency surgeons in June 2020 around the world, investigating the impact of SARS-CoV-2 pandemic on patients and septic diseases both requiring emergency surgery and the time-to-intervention in emergency surgery routine, as well as experiences with surgery in COVID-19 patients.
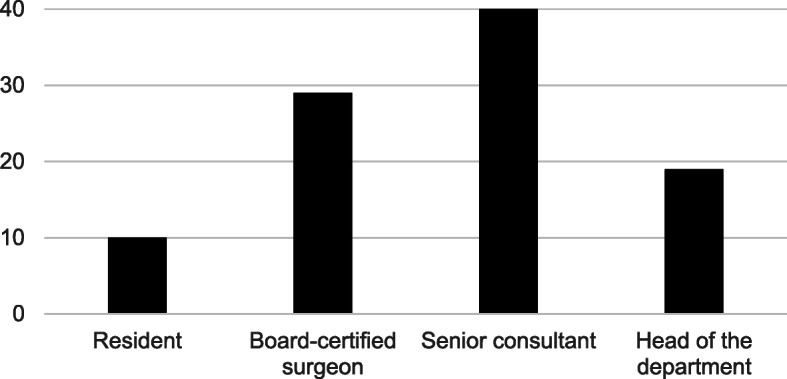
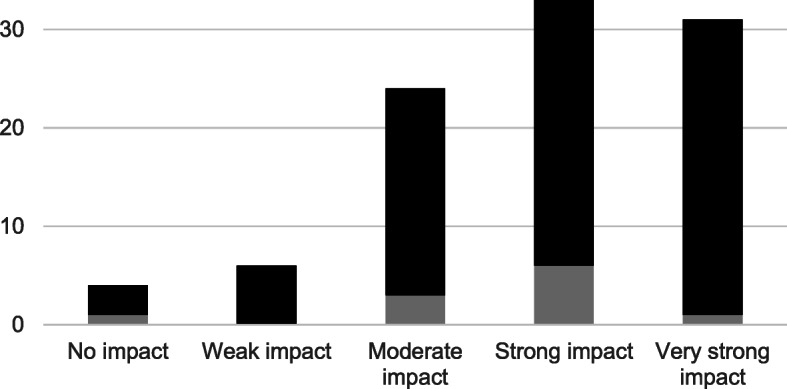
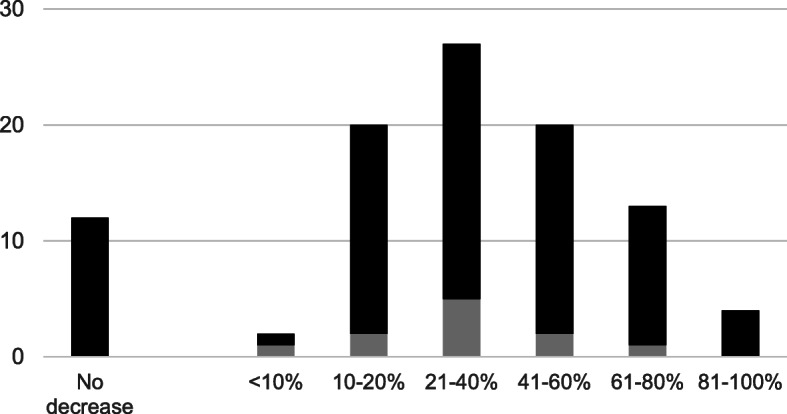
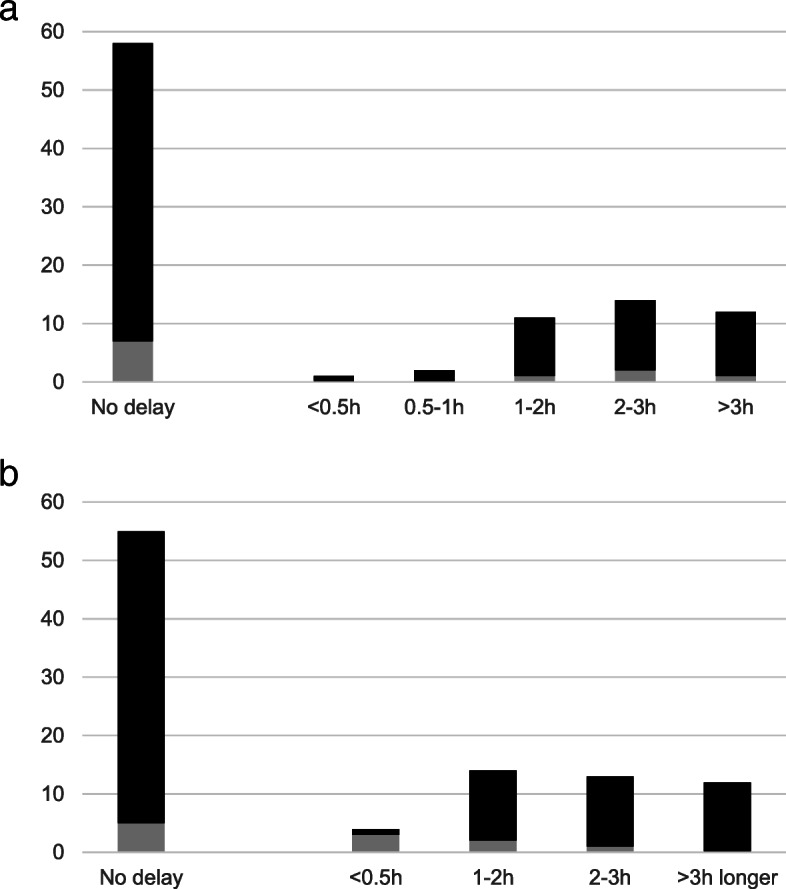
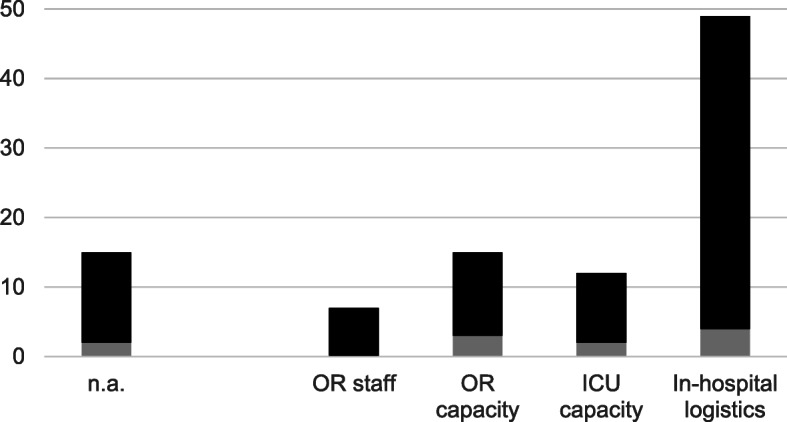
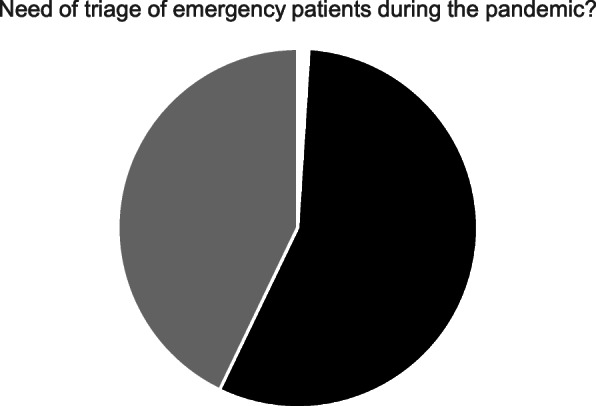
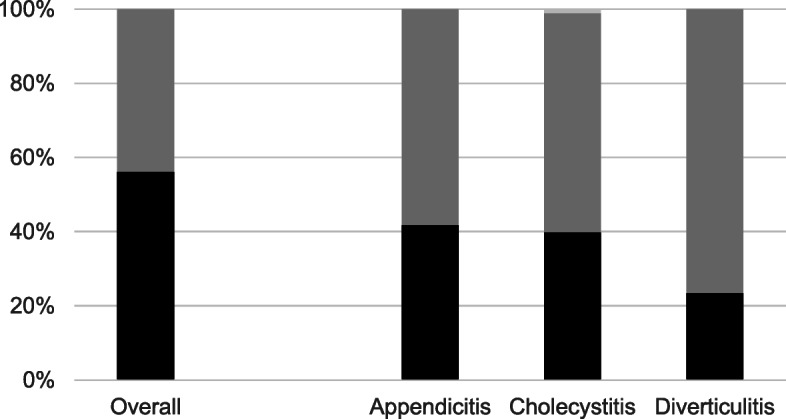
Results: Ninety-eight collaborators from 31 countries responded to the survey. The majority (65.3%) estimated the impact of the SARS-CoV-2 pandemic on emergency surgical patient care as being strong or very strong. Due to the pandemic, 87.8% reported a decrease in the total number of patients undergoing emergency surgery and approximately 25% estimated a delay of more than 2 h in the time-to-diagnosis and another 2 h in the time-to-intervention. Fifty percent make structural problems with in-hospital logistics (e.g. transport of patients, closed normal wards etc.) mainly responsible for delayed emergency surgery and the frequent need (56.1%) for a triage of emergency surgical patients. 56.1% of the collaborators observed more severe septic abdominal diseases during the pandemic, especially for perforated appendicitis and severe septic cholecystitis (41.8% and 40.2%, respectively). 62.2% had experiences with surgery in COVID-19-infected patients.
Conclusions: The results of The WSES COVID-19 emergency surgery survey are alarming. The combination of an estimated decrease in numbers of emergency surgical patients and an observed increase in more severe septic diseases may be a result of the fear of patients from infection with COVID-19 and a consecutive delayed hospital admission and diagnosis. A critical delay in time-to-diagnosis and time-to-intervention may be a result of changes in in-hospital logistics and operating room as well as intensive care capacities. Both reflect the potentially harmful impact of SARS-CoV-2 pandemic on emergency surgery services.
Keywords: Appendicitis; COVID-19; Cholecystitis; Emergency surgery; SARS-CoV-2; WSES.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
