

Mobilization of pre-existing polyclonal T cells specific to neoantigens but not self-antigens during treatment of a patient with melanoma with bempegaldesleukin and nivolumab
- PMID: 33298619
- PMCID: PMC7733177
- DOI: 10.1136/jitc-2020-001591
Mobilization of pre-existing polyclonal T cells specific to neoantigens but not self-antigens during treatment of a patient with melanoma with bempegaldesleukin and nivolumab
Erratum in
-
Correction: Mobilization of pre-existing polyclonal T cells specific to neoantigens but not self-antigens during treatment of a patient with melanoma with bempegaldesleukin and nivolumab.J Immunother Cancer. 2021 Feb;9(2):e001591corr1. doi: 10.1136/jitc-2020-001591corr1. J Immunother Cancer. 2021. PMID: 33526608 Free PMC article. No abstract available.
Abstract
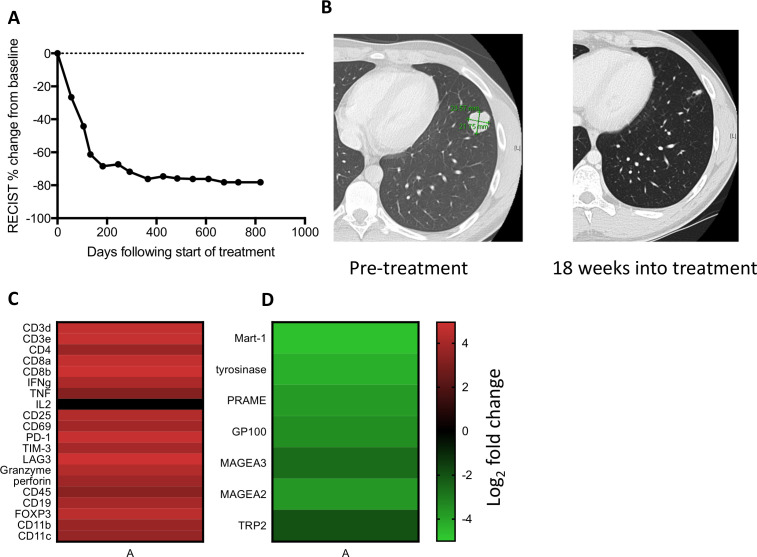
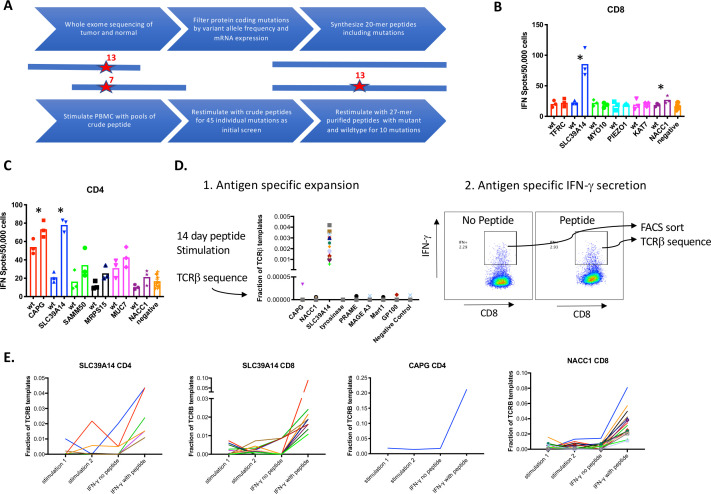
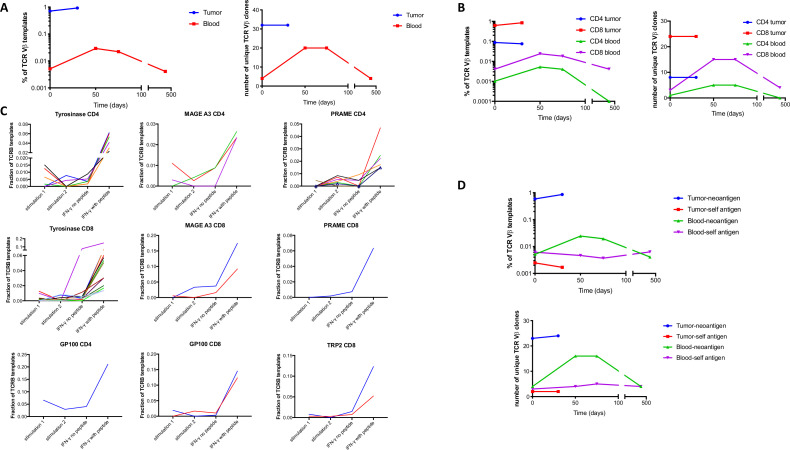
T cells that recognize self-antigens and mutated neoantigens are thought to mediate antitumor activity of immune checkpoint blockade (ICB) in melanoma. Few studies have analyzed self and neoantigen-specific T cell responses in patients responding to ICB. Here, we report a patient with metastatic melanoma who had a durable clinical response after treatment with the programmed cell death protein 1 inhibitor, nivolumab, combined with the first-in-class CD122-preferential interleukin-2 pathway agonist, bempegaldesleukin (BEMPEG, NKTR-214). We used a combination of antigen-specific T cell expansion and measurement of interferon-γ secretion to identify multiple CD4+ and CD8+ T cell clones specific for neoantigens, lineage-specific antigens and cancer testis antigens in blood and tumor from this patient prior to and after therapy. Polyclonal CD4+ and CD8+ T cells specific to multiple neoantigens but not self-antigens were highly enriched in pretreatment tumor compared with peripheral blood. Neoantigen, but not self-antigen-specific T cell clones expanded in frequency in the blood during successful treatment. There was evidence of dramatic immune infiltration into the tumor on treatment, and a modest increase in the relative frequency of intratumoral neoantigen-specific T cells. These observations suggest that diverse CD8+ and CD4+ T cell clones specific for neoantigens present in tumor before treatment had a greater role in immune tumor rejection as compared with self-antigen-specific T cells in this patient. Trial registration number: NCT02983045.
Keywords: T-lymphocytes; antigens; melanoma; neoplasm.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JRV, BJ and SR have equity interest in Lyell Immunopharma, and JZ and EE are employees of Nektar therapeutics, and this paper discusses use of an investigational drug owned by Nektar therapeutics.
Figures

References
-
- Anagnostou V, Smith KN, Forde PM, et al. Evolution of neoantigen landscape during immune checkpoint blockade in non-small cell lung cancer. Cancer Discov 2017;7:264–76. 10.1158/2159-8290.CD-16-0828 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials