

A blinded, controlled trial of objective measurement in Parkinson's disease
- PMID: 33298955
- PMCID: PMC7680151
- DOI: 10.1038/s41531-020-00136-9
A blinded, controlled trial of objective measurement in Parkinson's disease
Abstract
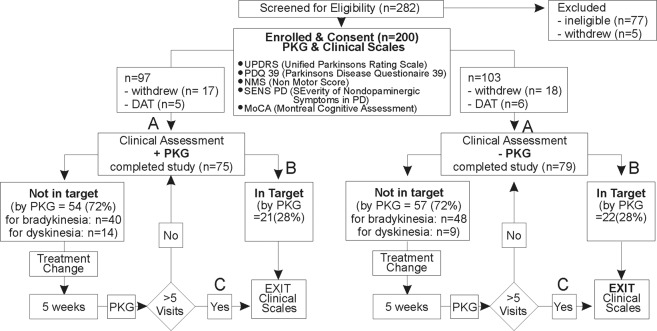
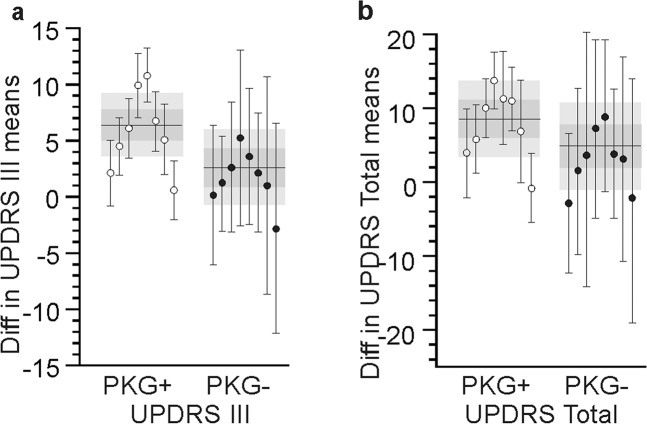
Medical conditions with effective therapies are usually managed with objective measurement and therapeutic targets. Parkinson's disease has effective therapies, but continuous objective measurement has only recently become available. This blinded, controlled study examined whether management of Parkinson's disease was improved when clinical assessment and therapeutic decisions were aided by objective measurement. The primary endpoint was improvement in the Movement Disorder Society-United Parkinson's Disease Rating Scale's (MDS-UPDRS) Total Score. In one arm, objective measurement assisted doctors to alter therapy over successive visits until objective measurement scores were in target. Patients in the other arm were conventionally assessed and therapies were changed until judged optimal. There were 75 subjects in the objective measurement arm and 79 in the arm with conventional assessment and treatment. There were statistically significant improvements in the moderate clinically meaningful range in the MDS-UPDRS Total, III, IV scales in the arm using objective measurement, but not in the conventionally treated arm. These findings show that global motor and non-motor disability is improved when management of Parkinson's disease is assisted by objective measurement.
Conflict of interest statement
M.K.H. is the inventor of the P.K.G. and is a paid consultant to G.K.C. (the manufacturer of the P.K.G.) to develop new products for the P.K.G. M.K.H. did not receive any personal or laboratory funding to undertake this study. The study, sponsored by the Florey Institute of Neurosciences and Mental Health, was investigator initiated, designed and led. The study was administered and conducted by staff from the Florey, and G.K.C. (the manufacturer of the P.K.G.) had no influence on the conduct of this study or the writing of this manuscript. It did not provide funding other than in kind gift of the P.K.G. loggers. K.E.K. and M.K.H. have financial interest in G.K.C. H.W. and C.V.F. were funded from the grants to undertake this study.
Figures



References
-
- Farzanehfar, P., Braybrook, M., Kotschet, K. & Horne, M. Objective measurement in clinical care of patients with parkinson’s disease: an RCT using the PKG. In 20th International Congress of Parkinons’ Disorders and Movement Disorders. Berlin, Germany (2016).
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
