

Prediction of breast cancer molecular subtypes using radiomics signatures of synthetic mammography from digital breast tomosynthesis
- PMID: 33299040
- PMCID: PMC7726048
- DOI: 10.1038/s41598-020-78681-9
Prediction of breast cancer molecular subtypes using radiomics signatures of synthetic mammography from digital breast tomosynthesis
Abstract
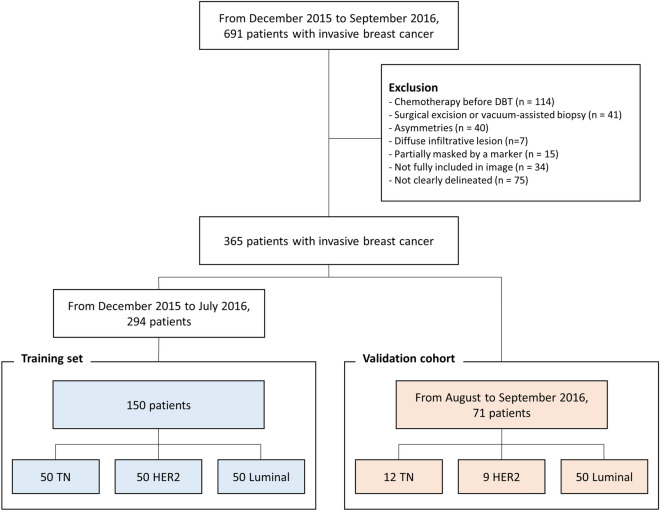
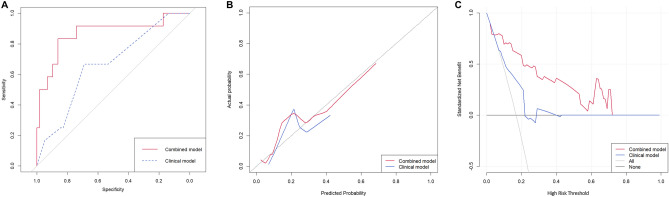
We aimed to predict molecular subtypes of breast cancer using radiomics signatures extracted from synthetic mammography reconstructed from digital breast tomosynthesis (DBT). A total of 365 patients with invasive breast cancer with three different molecular subtypes (luminal A + B, luminal; HER2-positive, HER2; triple-negative, TN) were assigned to the training set and temporally independent validation cohort. A total of 129 radiomics features were extracted from synthetic mammograms. The radiomics signature was built using the elastic-net approach. Clinical features included patient age, lesion size and image features assessed by radiologists. In the validation cohort, the radiomics signature yielded an AUC of 0.838, 0.556, and 0.645 for the TN, HER2 and luminal subtypes, respectively. In a multivariate analysis, the radiomics signature was the only independent predictor of the molecular subtype. The combination of the radiomics signature and clinical features showed significantly higher AUC values than clinical features only for distinguishing the TN subtype. In conclusion, the radiomics signature showed high performance for distinguishing TN breast cancer. Radiomics signatures may serve as biomarkers for TN breast cancer and may help to determine the direction of treatment for these patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
