

Assessment of physiological signs associated with COVID-19 measured using wearable devices
- PMID: 33299095
- PMCID: PMC7705652
- DOI: 10.1038/s41746-020-00363-7
Assessment of physiological signs associated with COVID-19 measured using wearable devices
Abstract
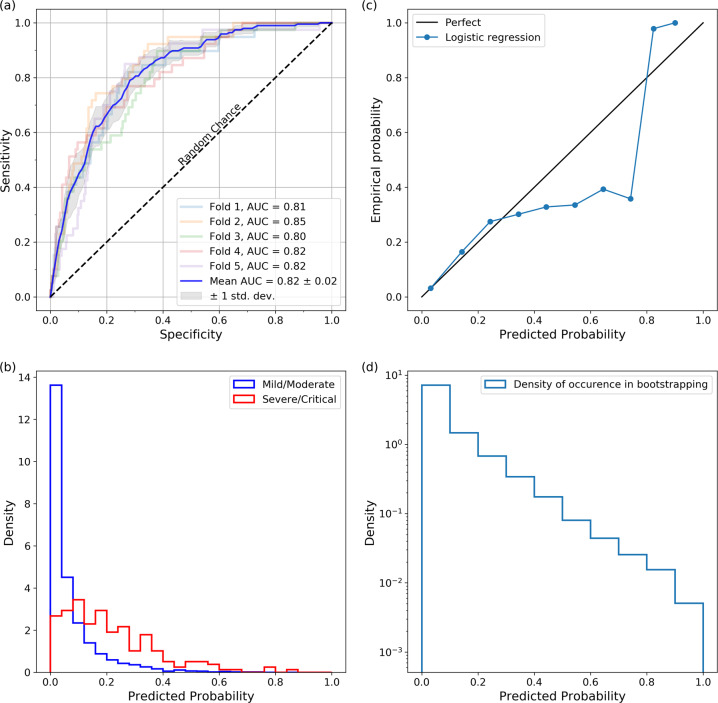
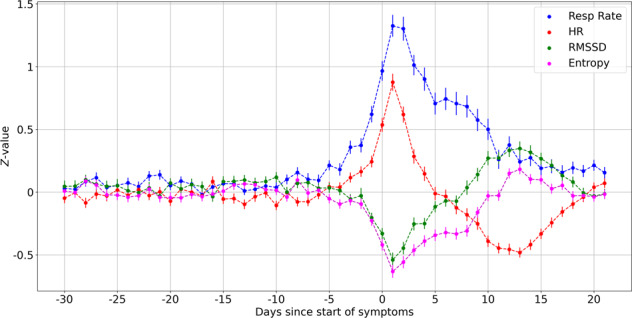
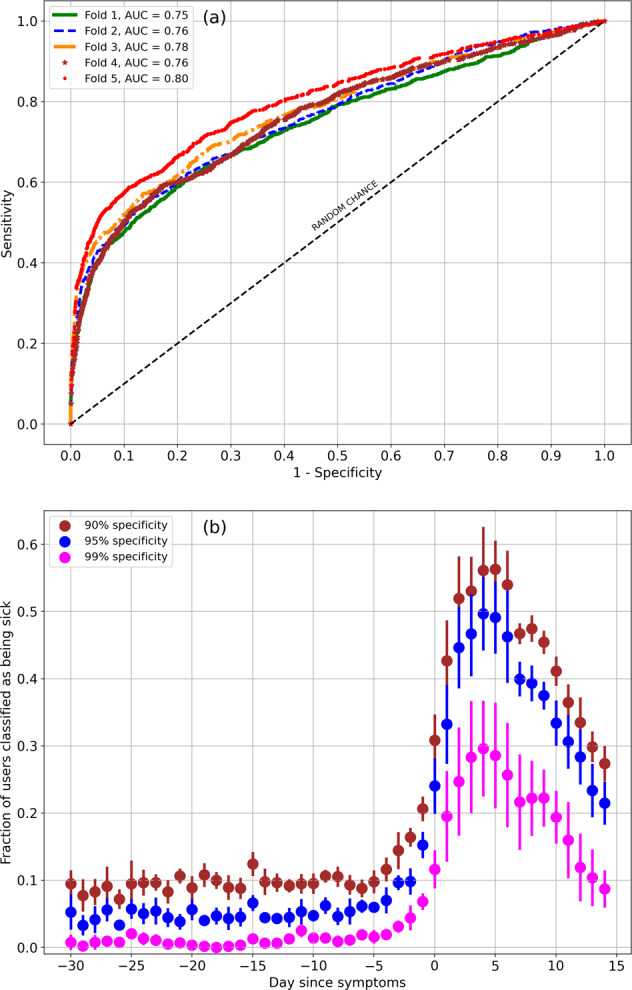
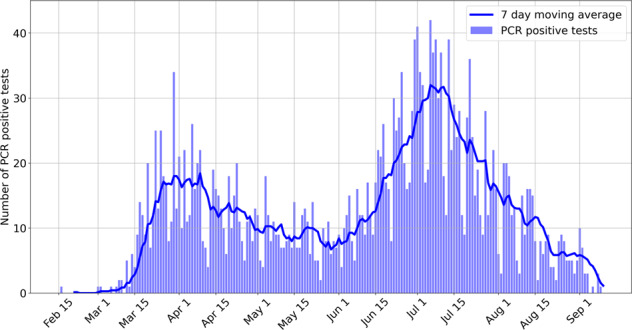
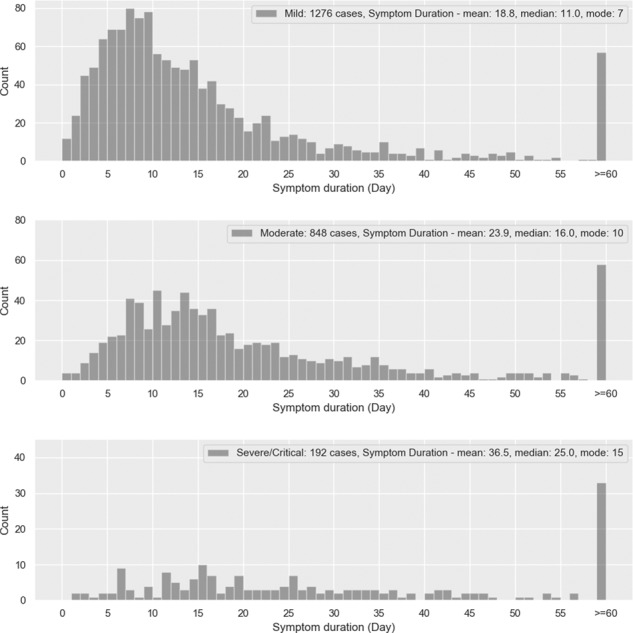
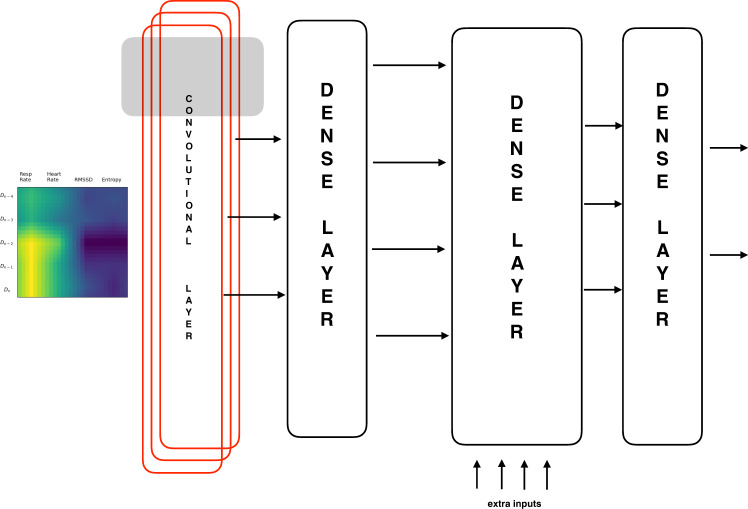
Respiration rate, heart rate, and heart rate variability (HRV) are some health metrics that are easily measured by consumer devices, which can potentially provide early signs of illness. Furthermore, mobile applications that accompany wearable devices can be used to collect relevant self-reported symptoms and demographic data. This makes consumer devices a valuable tool in the fight against the COVID-19 pandemic. Data on 2745 subjects diagnosed with COVID-19 (active infection, PCR test) were collected from May 21 to September 11, 2020, consisting of PCR positive tests conducted between February 16 and September 9. Considering male (female) participants, 11.9% (11.2%) of the participants were asymptomatic, 48.3% (47.8%) recovered at home by themselves, 29.7% (33.7%) recovered at home with the help of someone else, 9.3% (6.6%) required hospitalization without ventilation, and 0.5% (0.4%) required ventilation. There were a total of 21 symptoms reported, and the prevalence of symptoms varies by sex. Fever was present in 59.4% of male subjects and in 52% of female subjects. Based on self-reported symptoms alone, we obtained an AUC of 0.82 ± 0.017 for the prediction of the need for hospitalization. Based on physiological signs, we obtained an AUC of 0.77 ± 0.018 for the prediction of illness on a specific day. Respiration rate and heart rate are typically elevated by illness, while HRV is decreased. Measuring these metrics, taken in conjunction with molecular-based diagnostics, may lead to better early detection and monitoring of COVID-19.
Conflict of interest statement
All authors are funded by Fitbit Inc. The authors have no non-financial competing interests.
Figures
References
-
- Jensen MM, Kellett JG, Hallas P, Brabrand M. Fever increases heart rate and respiratory rate; a prospective observational study of acutely admitted medical patients. Acute Med. 2019;18:141–143. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
