

Comment
doi: 10.1038/s41375-020-01103-2.
Epub 2020 Dec 9.
SARS-CoV-2 antibody responses in patients with acute leukaemia
Affiliations
- PMID: 33299142
- PMCID: PMC7724438
- DOI: 10.1038/s41375-020-01103-2
Item in Clipboard
Comment
SARS-CoV-2 antibody responses in patients with acute leukaemia
Leukemia.
2021 Jan.
No abstract available
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
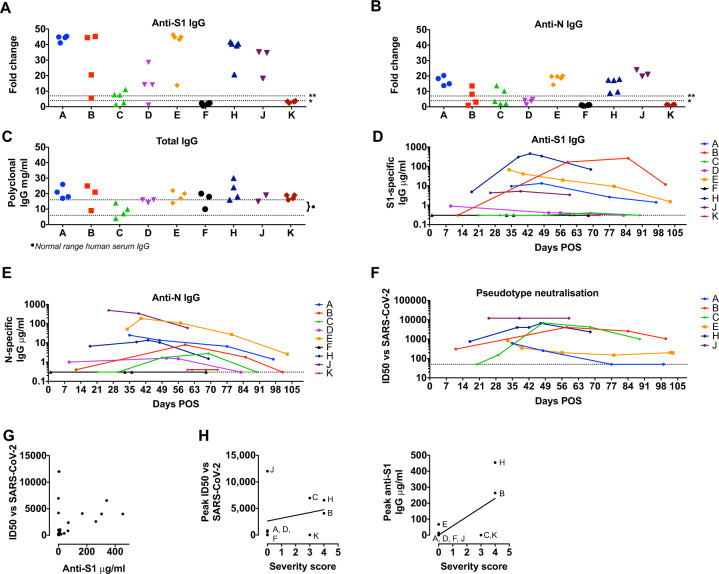
Serum samples from patients A–K were assayed on ELISA plates pre-coated with S1 (a) or N (b). Antigen production and assay conditions were as previously described [–6] except that all samples were treated with 0.5% NP40 before dilution in ELISA buffer. Absorbance was measured at 405 nm and data expressed as fold-change above blank background. The limit of detection (seropositivity) was determined as fold change >4 and is indicated by the dotted line marked *. The dotted line marked ** indicates the limit of quantification in the assay depicted in d–e, determined by the linear range of the standard curve. c ELISA plates were coated overnight at 4 °C with goat anti-human F(ab)’2. Serum samples from patients A–K, and commercial polyclonal IgG standard, were titrated in ELISA buffer and added to the ELISA plate. Binding was detected with goat anti-human IgG conjugated to peroxidase and absorbance read at 450 nm. IgG concentrations in serum were calculated based on interpolation from the IgG standard results using a four-parameter logistic (4PL) regression curve fitting model. Dotted lines marked with }* indicate the normal average range for IgG in human serum. d, e Sera supplemented with 0.5% NP40 from patients A–K were diluted in ELISA buffer and then added to a blocked ELISA plates pre-coated with the indicated antigen and three lanes of goat anti-human F(ab)’2 as per (c). Binding was detected with anti-IgG conjugated to alkaline phosphatase and absorbance measured at 405 nm. Antigen-specific IgG concentrations in serum were calculated based on interpolation from the IgG standard results using a four-parameter logistic (4PL) regression curve fitting model. The dotted line indicates the limit of quantification, which is determined by the linear range of the standard curve and higher than the limit of detection in a and b. f. Sequential serum samples from seropositive patients were titrated in duplicate and pre-incubated with luciferase-encoding HIV pseudotyped with the SARS-CoV-2 Spike for 1 h prior to the addition of HeLa cells expressing human ACE2 as previously described [7]. ID50 titres were only calculated in GraphPad Prism where at least two data points exhibited >50% neutralisation. ID50 values for each patient are plotted on the y-axis against days POS on the x-axis. g. ID50 values plotted against semi-quantitative S1 titres (μg/ml) for each sample. There is a trend to increasing ID50 with higher S1 titres but linear regression does not show a significant correlation (r = 0.06915, p = 0.0925). All data are from at least three independent experiments. h ID50 values and anti-S1 (μg/ml) values plotted against COVID-19 severity score for each patient as cited in Table 1. A trend line is shown but there were insufficient sample numbers to assess correlation and significance.
Comment in
-
Seroconversion and dynamics of the anti-SARS-CoV-2 antibody response related to a hospital COVID-19 outbreak among pediatric oncology patients.Leukemia. 2021 Jun;35(6):1820-1822. doi: 10.1038/s41375-021-01288-0. Epub 2021 May 18. Leukemia. 2021. PMID: 34007047 Free PMC article. No abstract available.
Comment on
-
Anti-SARS-CoV-2 antibody response in patients with chronic lymphocytic leukemia.Leukemia. 2020 Nov;34(11):3047-3049. doi: 10.1038/s41375-020-01030-2. Epub 2020 Aug 27. Leukemia. 2020. PMID: 32855439 Free PMC article. No abstract available.
References
-
- Passamonti F, Cattaneo C, Arcaini L, Bruna R, Cavo M, Merli F, et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: a retrospective, multicentre, cohort study. Lancet Haematol. 2020;10:e737–45. doi: 10.1016/S2352-3026(20)30251-9. - DOI - PMC - PubMed
-
- Zeidan AM, Boddu PC, Patnaik MM, Bewersdorf JP, Stahl M, Rampal RK, et al. Special considerations in the management of adult patients with acute leukaemias and myeloid neoplasms in the COVID-19 era: recommendations from a panel of international experts. Lancet Haematol. 2020;7:e601–12. doi: 10.1016/S2352-3026(20)30205-2. - DOI - PMC - PubMed
-
- Pickering S, Betancor G, Galao RP, Merrick B, Signell AW, Wilson HD, et al. Comparative assessment of multiple COVID-19 serological technologies supports continued evaluation of point-of-care lateral flow assays in hospital and community healthcare settings. PLoS Pathog. 2020;16:e1008817. doi: 10.1371/journal.ppat.1008817. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
