

Meta-analysis and meta-regression of outcomes for adult living donor liver transplantation versus deceased donor liver transplantation
- PMID: 33300241
- PMCID: PMC9048132
- DOI: 10.1111/ajt.16440
Meta-analysis and meta-regression of outcomes for adult living donor liver transplantation versus deceased donor liver transplantation
Abstract
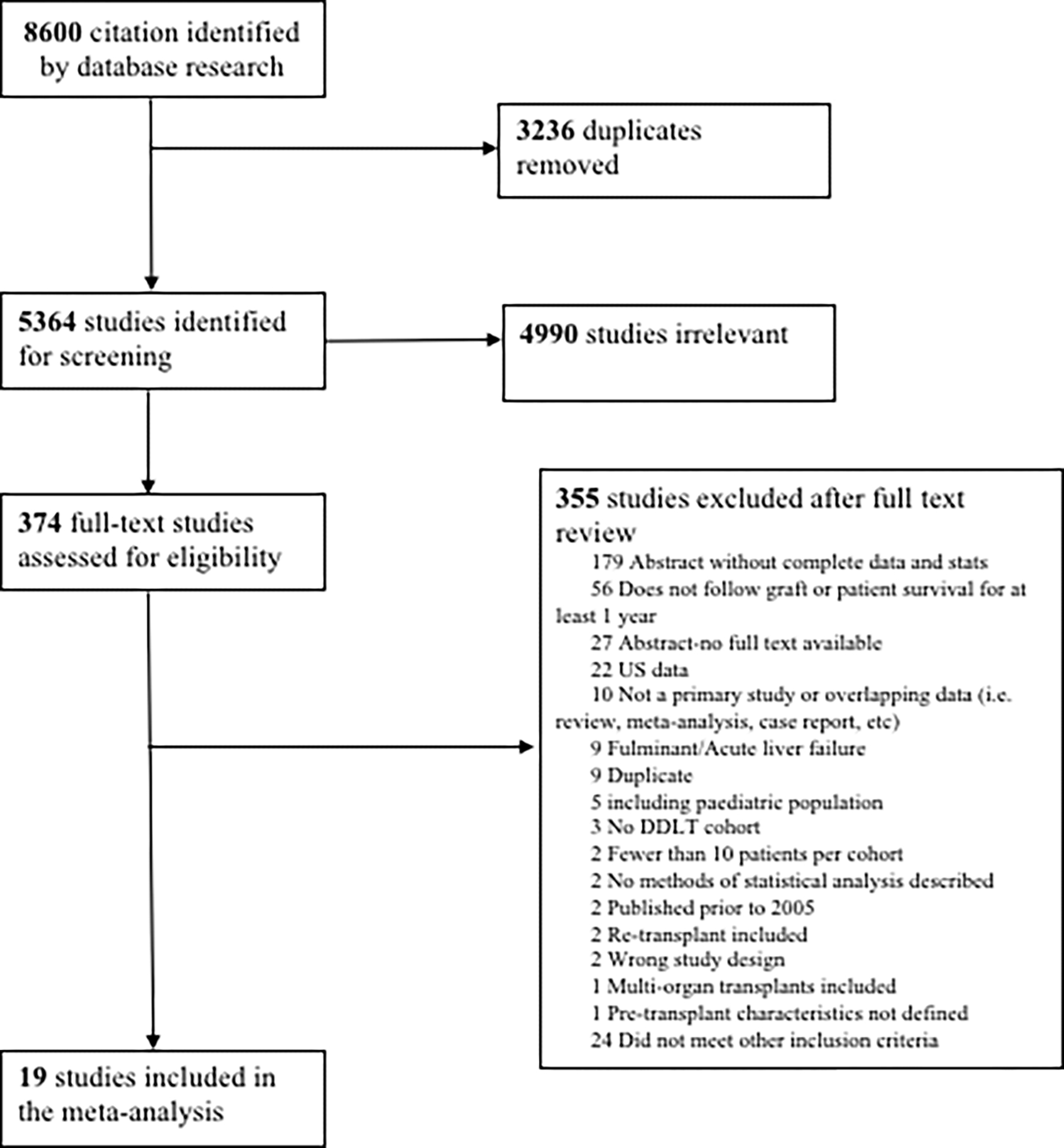
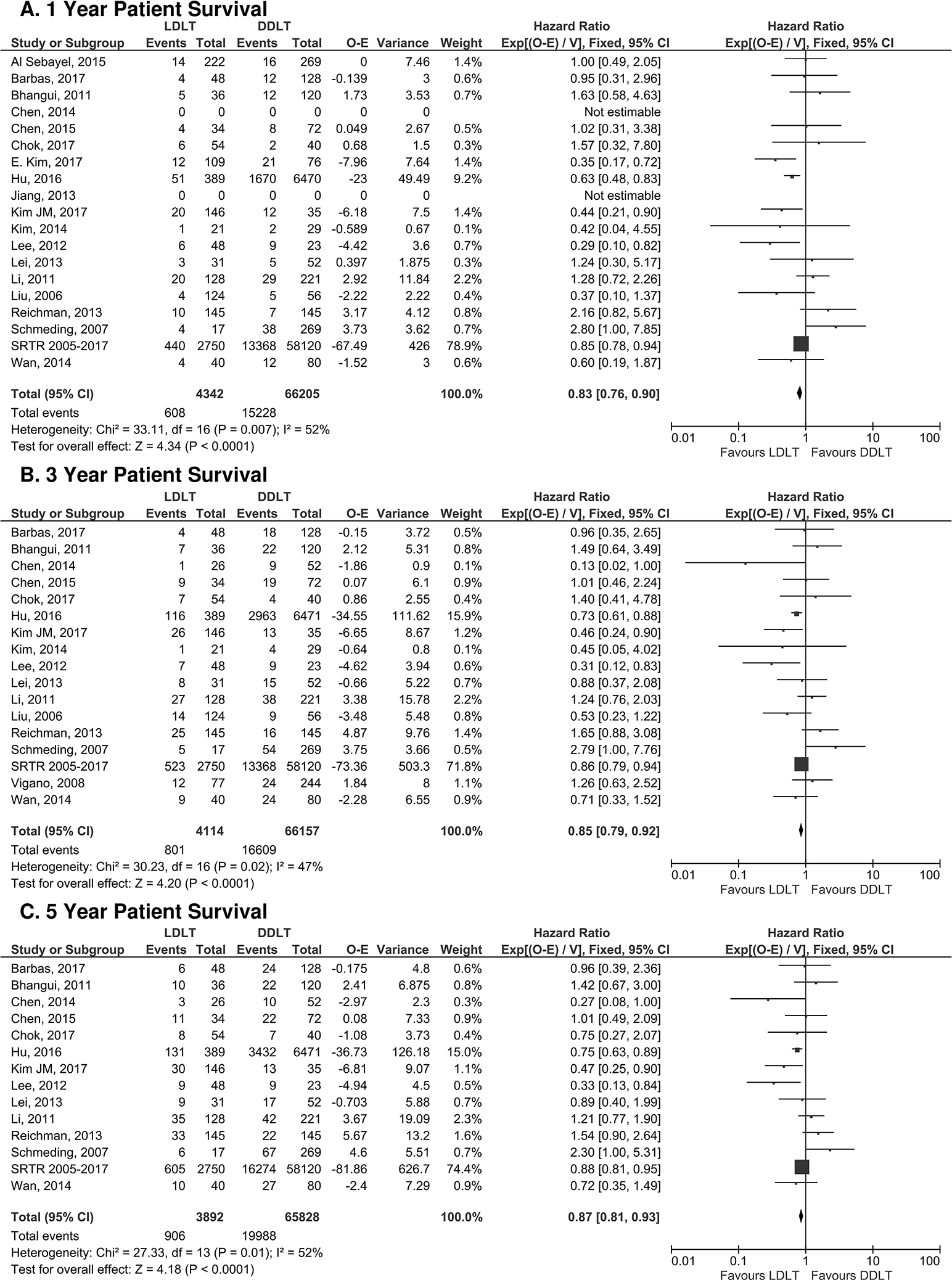
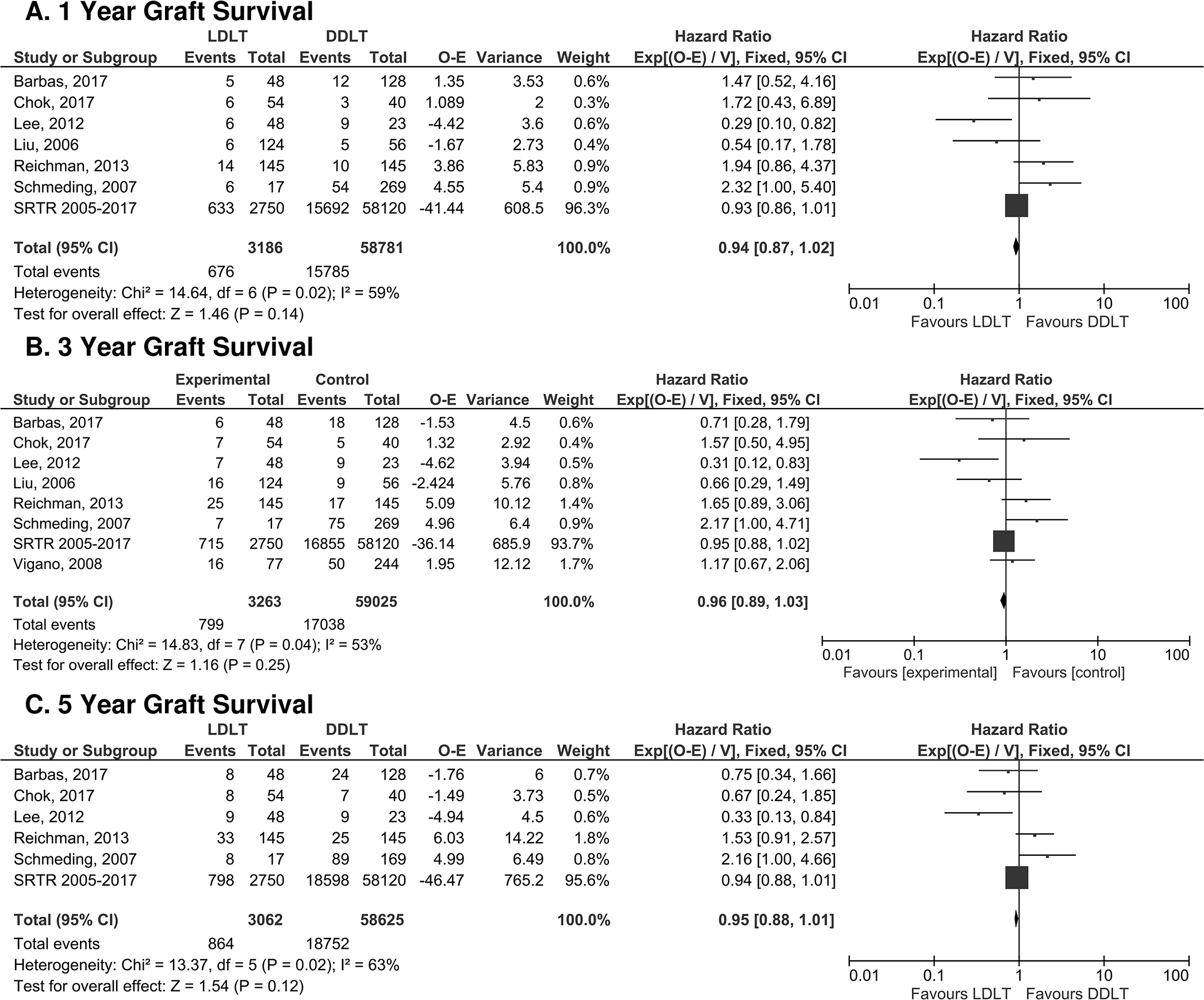
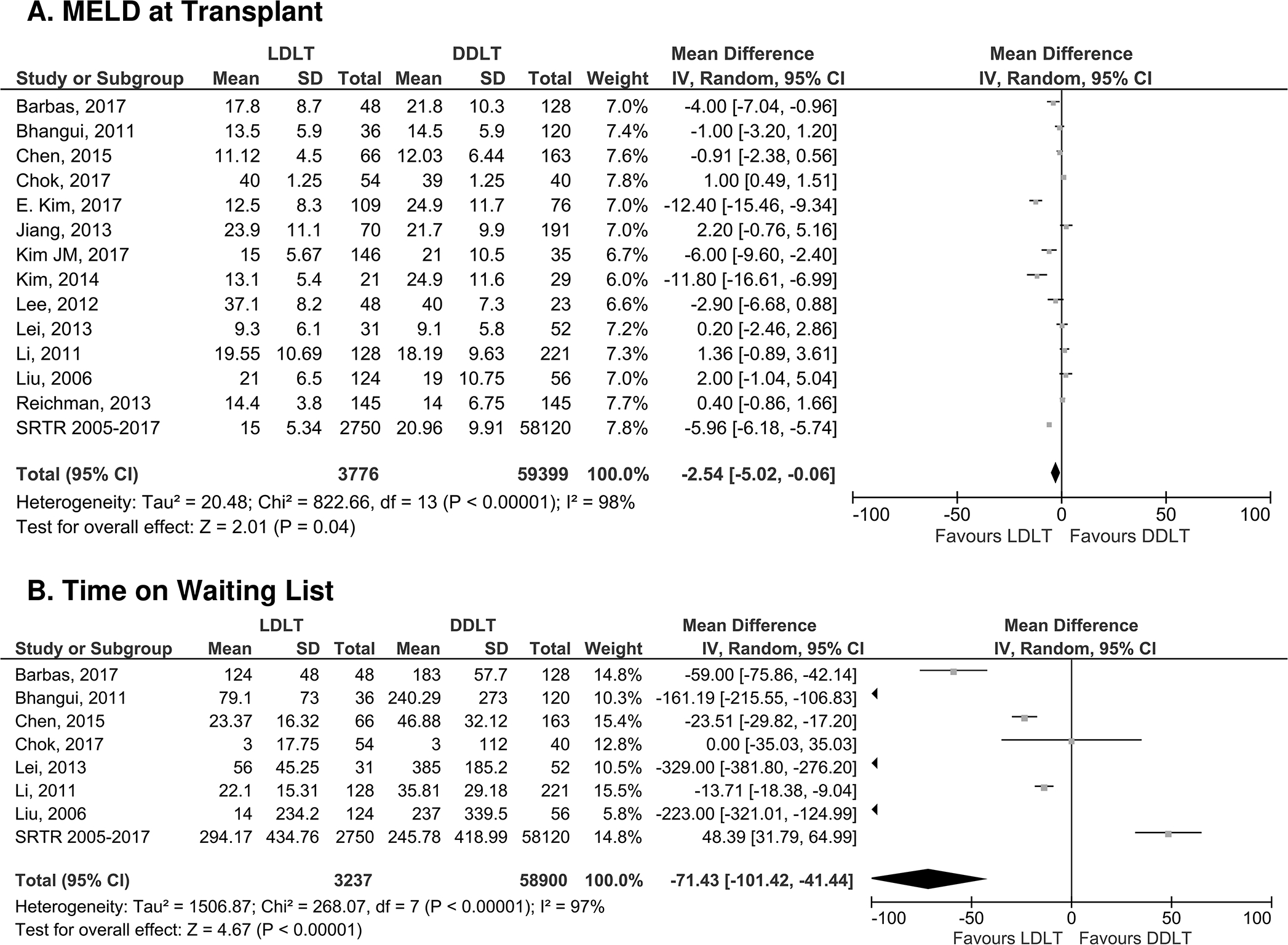
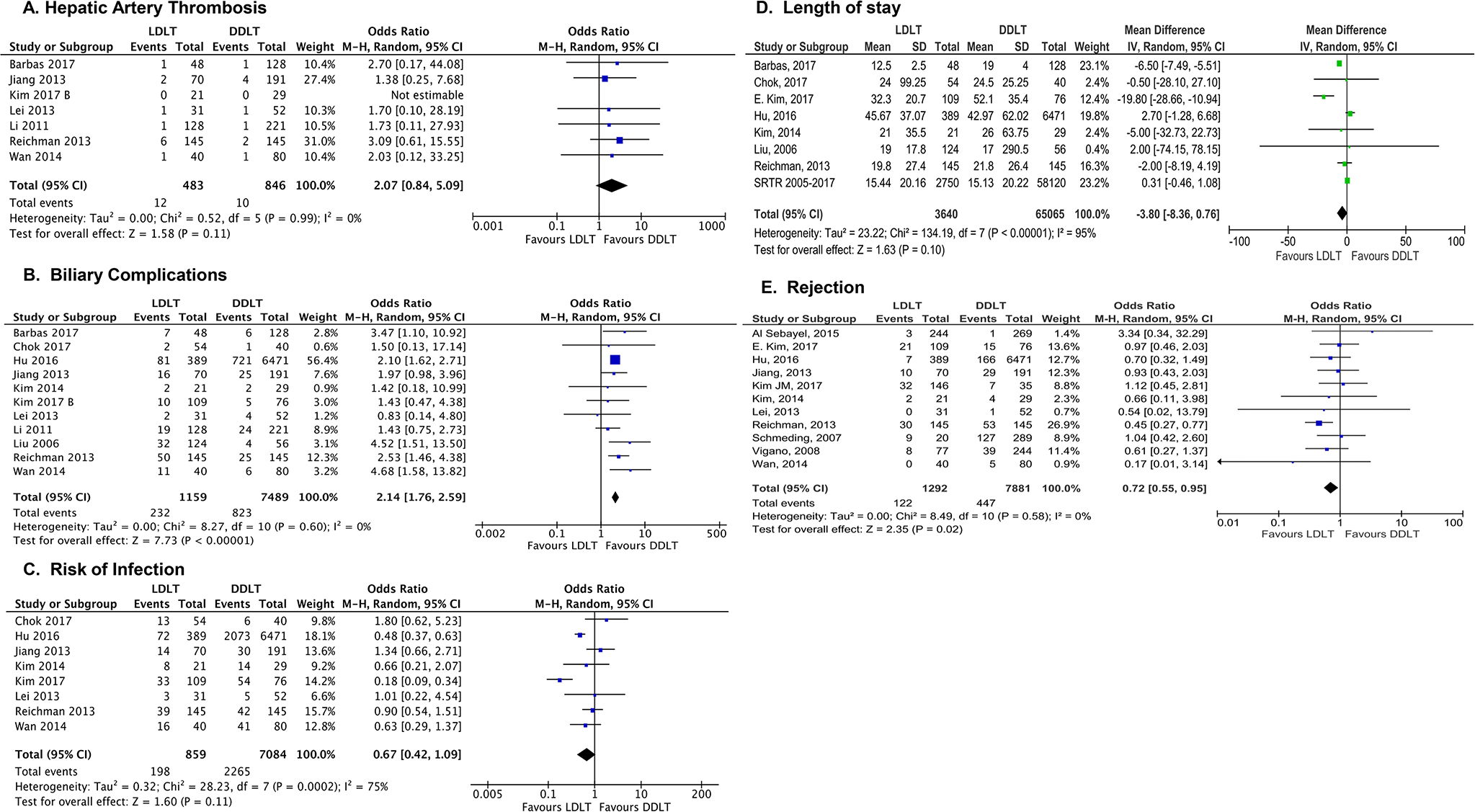
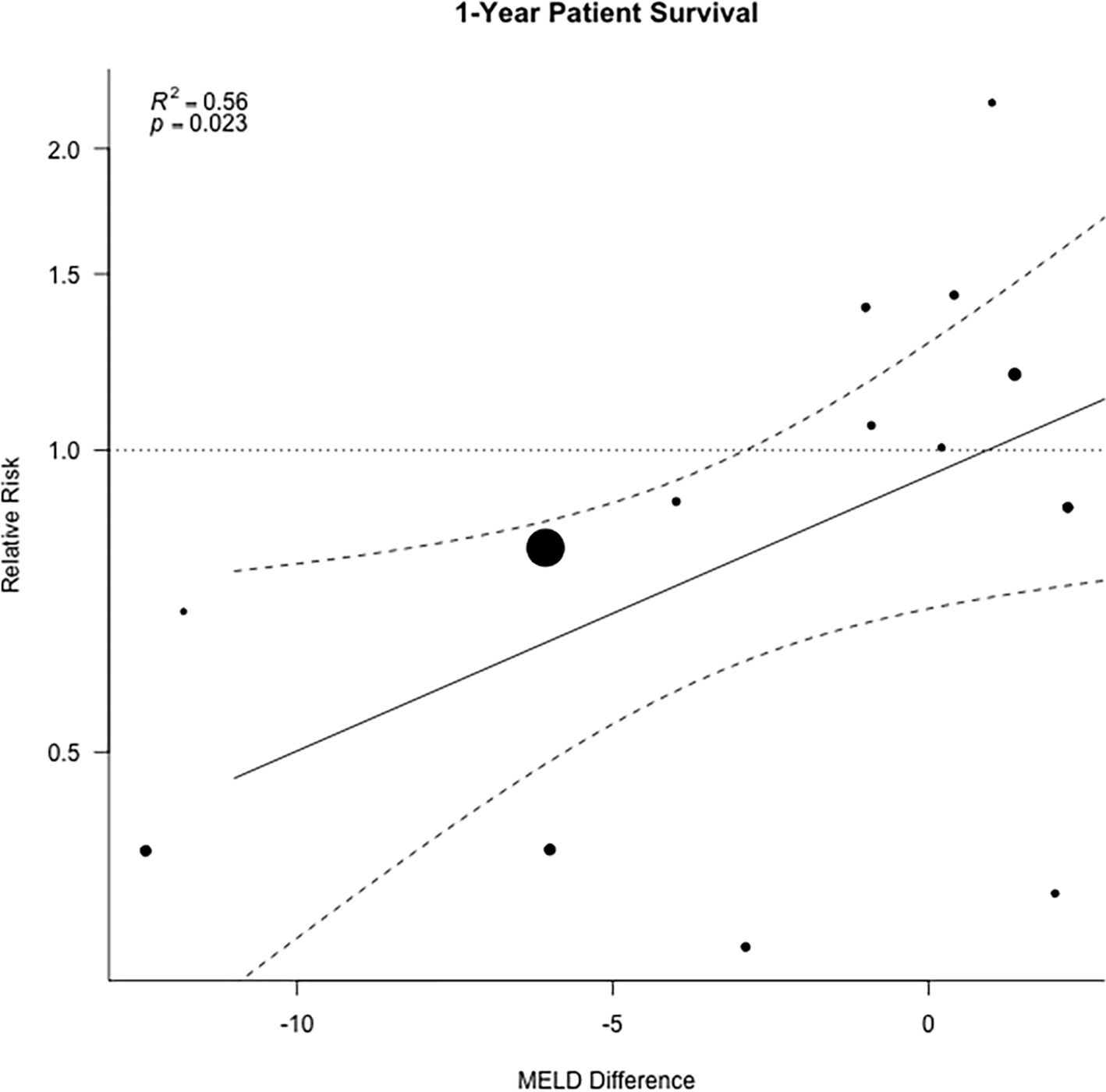
Prior single center or registry studies have shown that living donor liver transplantation (LDLT) decreases waitlist mortality and offers superior patient survival over deceased donor liver transplantation (DDLT). The aim of this study was to compare outcomes for adult LDLT and DDLT via systematic review. A meta-analysis was conducted to examine patient survival and graft survival, MELD, waiting time, technical complications, and postoperative infections. Out of 8600 abstracts, 19 international studies comparing adult LDLT and DDLT published between 1/2005 and 12/2017 were included. U.S. outcomes were analyzed using registry data. Overall, 4571 LDLT and 66,826 DDLT patients were examined. LDLT was associated with lower mortality at 1, 3, and 5 years posttransplant (5-year HR 0.87 [95% CI 0.81-0.93], p < .0001), similar graft survival, lower MELD at transplant (p < .04), shorter waiting time (p < .0001), and lower risk of rejection (p = .02), with a higher risk of biliary complications (OR 2.14, p < .0001). No differences were observed in rates of hepatic artery thrombosis. In meta-regression analysis, MELD difference was significantly associated with posttransplant survival (R2 0.56, p = .02). In conclusion, LDLT is associated with improved patient survival, less waiting time, and lower MELD at LT, despite posing a higher risk of biliary complications that did not affect survival posttransplant.
Keywords: clinical research / practice; liver transplantation / hepatology; liver transplantation: living donor; meta-analysis.
© 2020 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
Figures
References
-
- World Health Organization. GENERAL INFORMATION OF THE COUNTRY. Global Observatory on Donation and Transplantation. http://www.transplant-observatory.org/. Published 2020. Accessed March 3, 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
