

How I perform hematopoietic stem cell transplantation on patients with a history of invasive fungal disease
- PMID: 33301030
- PMCID: PMC7731790
- DOI: 10.1182/blood.2020005884
How I perform hematopoietic stem cell transplantation on patients with a history of invasive fungal disease
Abstract
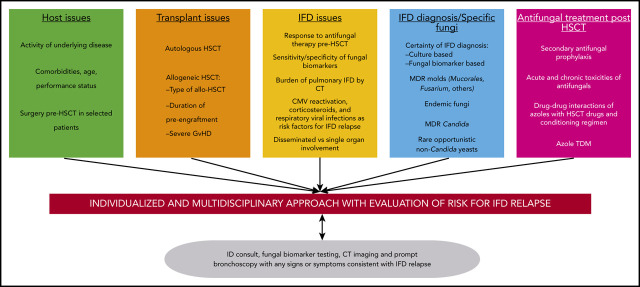
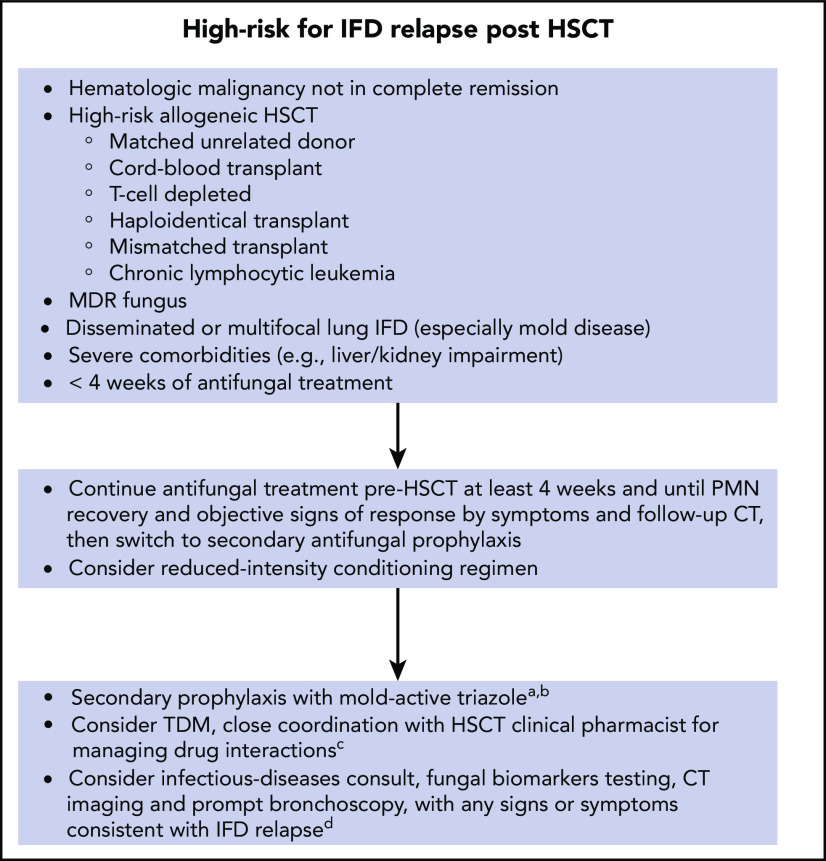
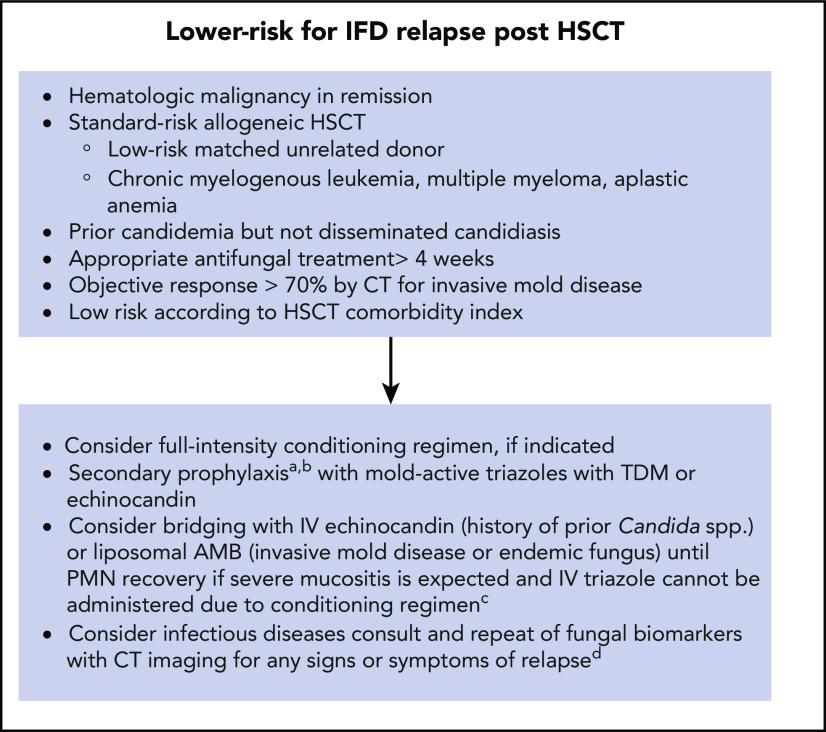
Hematopoietic transplantation is the preferred treatment for many patients with hematologic malignancies. Some patients may develop invasive fungal diseases (IFDs) during initial chemotherapy, which need to be considered when assessing patients for transplantation and treatment posttransplantation. Given the associated high risk of relapse and mortality in the post-hematopoietic stem cell transplantation (HSCT) period, IFDs, especially invasive mold diseases, were historically considered a contraindication for HSCT. Over the last 3 decades, advances in antifungal drugs and early diagnosis have improved IFD outcomes, and HSCT in patients with a recent IFD has become increasingly common. However, an organized approach for performing transplantation in patients with a prior IFD is scarce, and decisions are highly individualized. Patient-, malignancy-, transplantation procedure-, antifungal treatment-, and fungus-specific issues affect the risk of IFD relapse. Effective surveillance to detect IFD relapse post-HSCT and careful drug selection for antifungal prophylaxis are of paramount importance. Antifungal drugs have their own toxicities and interact with immunosuppressive drugs such as calcineurin inhibitors. Immune adjunct cytokine or cellular therapy and surgery can be considered in selected cases. In this review, we critically evaluate these factors and provide guidance for the complex decision making involved in the peri-HSCT management of these patients.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: P.P.-A. has received honoraria for talks on behalf of Pfizer. D.P.K. has received research support from Astellas and Gilead and has received honoraria from Merck, Astellas, Gilead, Cidara, and Mayne Pharmaceuticals. R.E.C. declares no competing financial interests.
Figures
References
-
- Chamilos G, Luna M, Lewis RE, et al. Invasive fungal infections in patients with hematologic malignancies in a tertiary care cancer center: an autopsy study over a 15-year period (1989-2003). Haematologica. 2006;91(7):986-989. - PubMed
-
- Pagano L, Caira M, Candoni A, et al. The epidemiology of fungal infections in patients with hematologic malignancies: the SEIFEM-2004 study. Haematologica. 2006;91(8):1068-1075. - PubMed
-
- Caillot D, Casasnovas O, Bernard A, et al. Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery. J Clin Oncol. 1997;15(1):139-147. - PubMed
-
- Greene RE, Schlamm HT, Oestmann J-W, et al. Imaging findings in acute invasive pulmonary aspergillosis: clinical significance of the halo sign. Clin Infect Dis. 2007;44(3):373-379. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
