

Loss of HER2 and decreased T-DM1 efficacy in HER2 positive advanced breast cancer treated with dual HER2 blockade: the SePHER Study
- PMID: 33302999
- PMCID: PMC7731769
- DOI: 10.1186/s13046-020-01797-3
Loss of HER2 and decreased T-DM1 efficacy in HER2 positive advanced breast cancer treated with dual HER2 blockade: the SePHER Study
Abstract
Background: HER2-targeting agents have dramatically changed the therapeutic landscape of HER2+ advanced breast cancer (ABC). Within a short time frame, the rapid introduction of new therapeutics has led to the approval of pertuzumab combined with trastuzumab and a taxane in first-line, and trastuzumab emtansine (T-DM1) in second-line. Thereby, evidence of T-DM1 efficacy following trastuzumab/pertuzumab combination is limited, with data from some retrospective reports suggesting lower activity. The purpose of the present study is to investigate T-DM1 efficacy in pertuzumab-pretreated and pertuzumab naïve HER2 positive ABC patients. We also aimed to provide evidence on the exposure to different drugs sequences including pertuzumab and T-DM1 in HER2 positive cell lines.
Methods: The biology of HER2 was investigated in vitro through sequential exposure of resistant HER2 + breast cancer cell lines to trastuzumab, pertuzumab, and their combination. In vitro experiments were paralleled by the analysis of data from 555 HER2 + ABC patients treated with T-DM1 and evaluation of T-DM1 efficacy in the 371 patients who received it in second line. Survival estimates were graphically displayed in Kaplan Meier curves, compared by log rank test and, when possibile, confirmed in multivariate models.
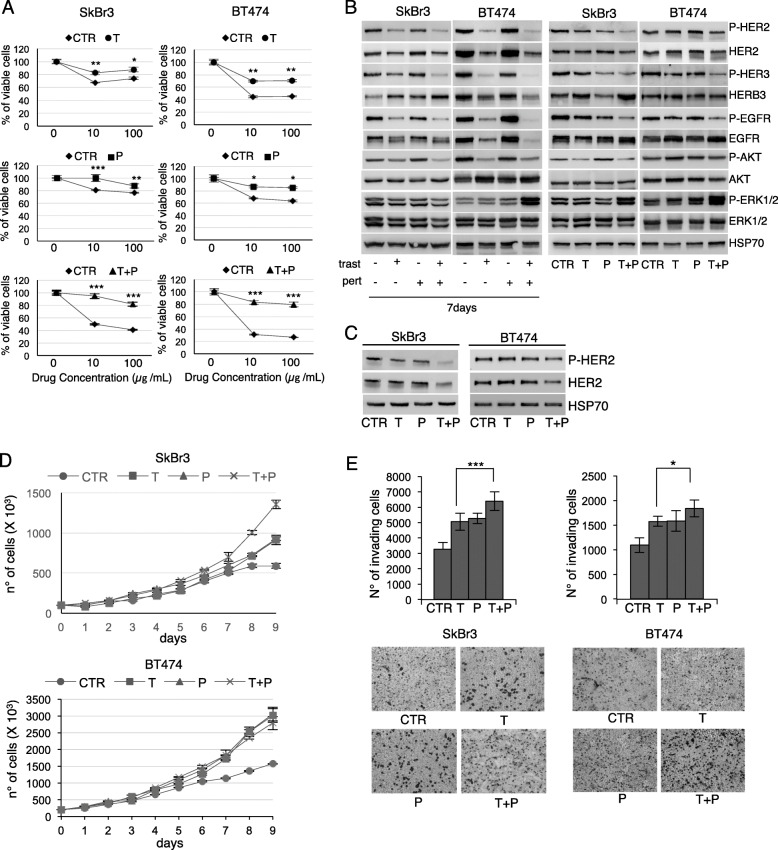
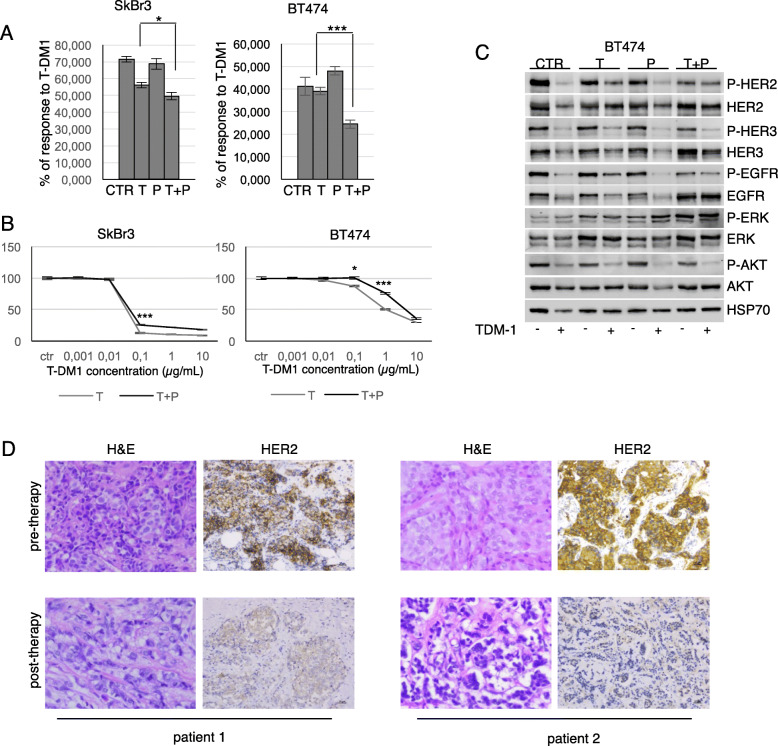
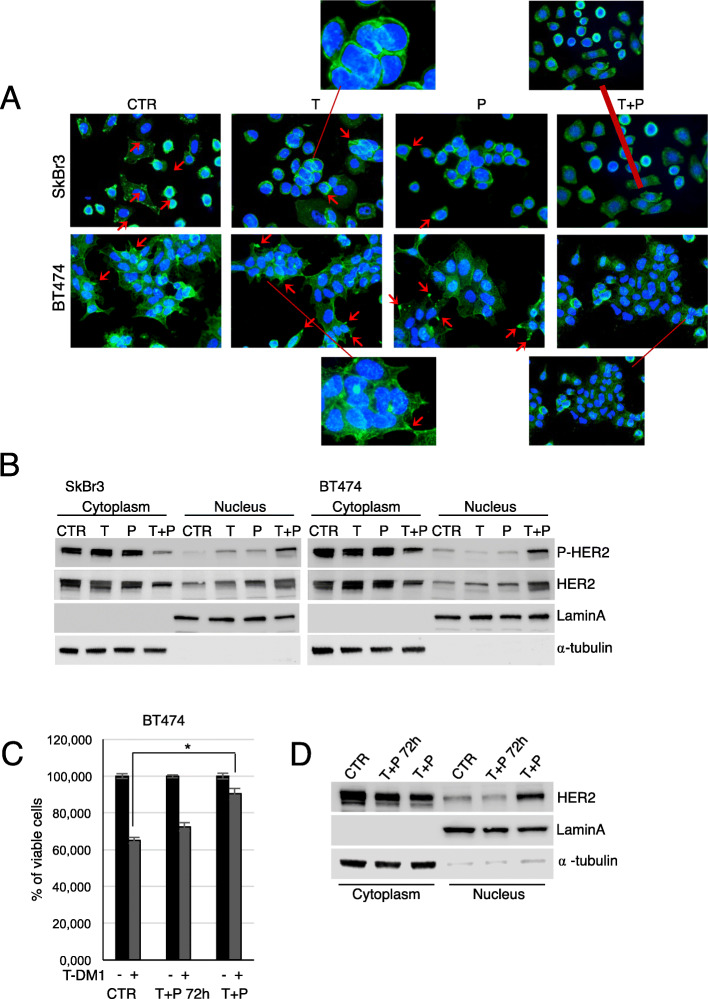
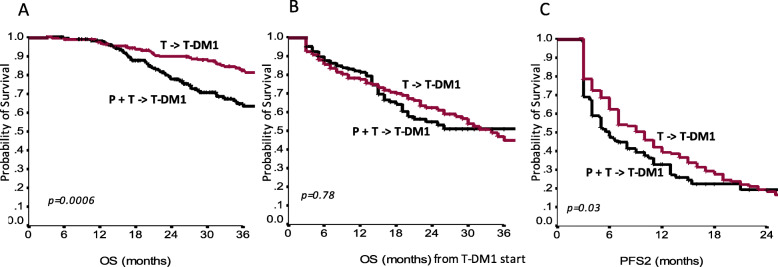
Results: We herein show evidence of lower activity of T-DM1 in two HER2+ breast cancer cell lines resistant to trastuzumab+pertuzumab, as compared to trastuzumab-resistant cells. Lower T-DM1 efficacy was associated with a marked reduction of HER2 expression on the cell membrane and its nuclear translocation. HER2 downregulation at the membrane level was confirmed in biopsies of four trastuzumab/pertuzumab-pretreated patients. Among the 371 patients treated with second-line T-DM1, median overall survival (mOS) from diagnosis of advanced disease and median progression-free survival to second-line treatment (mPFS2) were 52 and 6 months in 177 patients who received trastuzumab/pertuzumab in first-line, and 74 and 10 months in 194 pertuzumab-naïve patients (p = 0.0006 and 0.03 for OS and PFS2, respectively).
Conclusions: Our data support the hypothesis that the addition of pertuzumab to trastuzumab reduces the amount of available plasma membrane HER2 receptor, limiting the binding of T-DM1 in cancer cells. This may help interpret the less favorable outcomes of second-line T-DM1 in trastuzumab/pertuzumab pre-treated patients compared to their pertuzumab-naïve counterpart.
Keywords: HER2+ breast cancer; T-DM1 efficacy; Trastuzumab/pertuzumab blockade.
Conflict of interest statement
GB, RL, VL, EK, MB, MMS, RB, LL, CF, EC, DG, AC, VA, CZ, GT, GB, MM, DM, ST, PM, MRV, RM, MAF, NDO, EMV, DC, GS, FG, CG, PDM, MR, IS, AS, GC, RF, GS declare no conflicts of interest. LP received travel grants from Eisai, Roche, Pfizer, Novartis; speaker fees from Roche, Pfizer, Novartis, Gentili. CM has received personal consultancy fees from Bayer, Roche, Daiichi Sankyo, MSD. TG received travel grants from Eisai, Roche, Pfizer, Novartis; speaker fees/advisory boards from Roche, Pfizer, Novartis, Gentili, Lilly. CN received travel grants/personal fees from Pfizer, EISAI, Novartis, Merck Sharp &Dohme, AstraZeneca. NLV received personal fees from Eisai and Novartis; research funding from Eisai, travel grants from Pfizer, Roche, Gentili; consulting role from Celldex. Em.Br. is supported by the Italian Association for Cancer Research AIRC-IG 20583; he was supported by the International Association for Lung Cancer (IASLC), the LILT (LegaItaliana per la Lotta contro i Tumori) and Fondazione Cariverona; he received speakers’ and travels’ fee from MSD, Astra-Zeneca, Celgene, Pfizer, Helsinn, Eli-Lilly, BMS, Novartis and Roche; consultant’s fee from Roche, Pfizer; institutional research grants from Astra-Zeneca, Roche. Lu.Mos. received advisory board from Roche. An.Mic. received travel grants from Eisai, Celgene, Novartis, Ipsen; personal fees, advisory boards from EISAI, Novartis, Astra Zeneca, Teva, Pfizer, Celgene. A.R. received fees from Bristol, Pfizer, Bayer, Kyowa Kirin, Ambrosetti for advisory board activity; and speaker honorarium from Roche Diagnostics. OG received personal fees from Celgene, Novartis, Eisai; research funding from Eisai, consulting activities with Celgene, Eisai, Pfizer, Amgen. IP received personal fees/advisory boards from Roche, Pfizer, Novartis, Italfarmaco, Gentili, Pierre Fabre. MC received personal fees, advisory boards from Pierre Fabre, Astra Zeneca, Celgene, Eisai, Novartis, Lilly. RDM declares to be a scientific advisory board member at Exosomics SpA (Siena IT), Hibercell Inc. (New York, NY), Kiromic Inc. (Houston, TX) and at Exiris Inc. (Rome, IT). ADL received consulting fees from Novartis and Roche. PV received travel grants from Eisai, Roche, Pfizer, Novartis; speaker fees/advisory boards from Roche, Pfizer, Novartis, Gentili, Lilly.
Figures
References
-
- Marty M, Cognetti F, Maraninchi D, Snyder R, Mauriac L, Tubiana-Hulin M, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005;23:4265–4274. doi: 10.1200/JCO.2005.04.173. - DOI - PubMed
-
- Brufsky A. Trastuzumab-based therapy for patients with HER2-positive breast cancer: from early scientific development to foundation of care. Am J Clin Oncol. 2010;33:186–195. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
