

Evaluation of the health and healthcare system burden due to antimicrobial-resistant Escherichia coli infections in humans: a systematic review and meta-analysis
- PMID: 33303015
- PMCID: PMC7726913
- DOI: 10.1186/s13756-020-00863-x
Evaluation of the health and healthcare system burden due to antimicrobial-resistant Escherichia coli infections in humans: a systematic review and meta-analysis
Abstract
Background: Assessment of the burden of disease due to antimicrobial-resistant Escherichia coli infections facilitates understanding the scale of the problem and potential impacts, and comparison to other diseases, which allows prioritization of research, surveillance, and funding. Using systematic review and meta-analysis methodology, the objectives were to evaluate whether humans with antimicrobial-resistant E. coli infections experience increases in measures of health or healthcare system burden when compared to susceptible E. coli infections.
Methods: Comprehensive literature searches were performed in four primary and seven grey literature databases. Analytic observational studies of human E. coli infections that assessed the impact of resistance to third/fourth/fifth-generation cephalosporins, resistance to quinolones, and/or multidrug resistance on mortality, treatment failure, length of hospital stay and/or healthcare costs were included. Two researchers independently performed screening, data extraction, and risk of bias assessment. When possible, random effect meta-analyses followed by assessment of the confidence in the cumulative evidence were performed for mortality and length of hospital stay outcomes, and narrative syntheses were performed for treatment failure and healthcare costs.
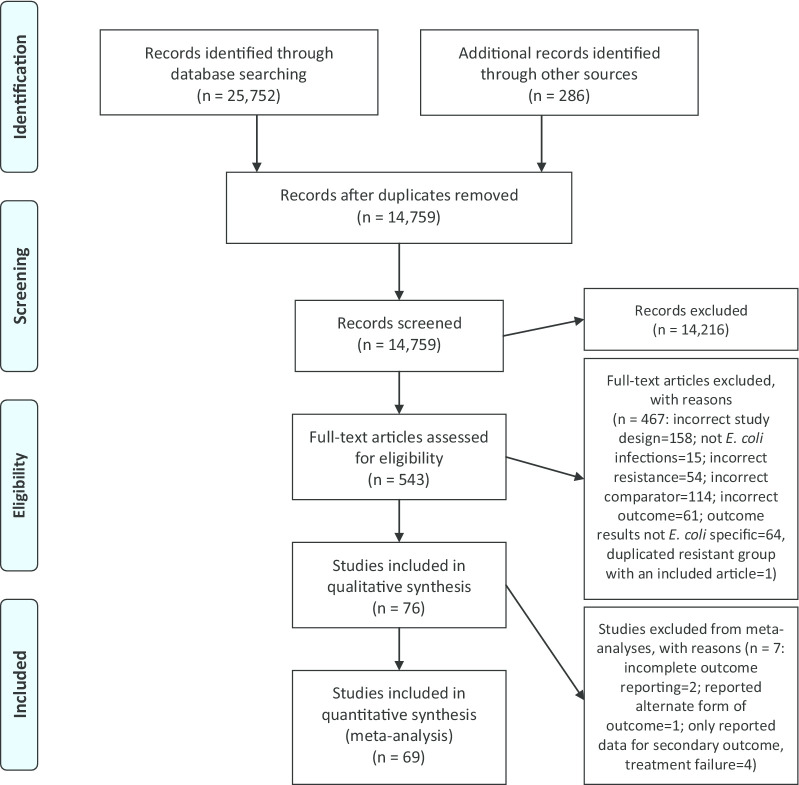
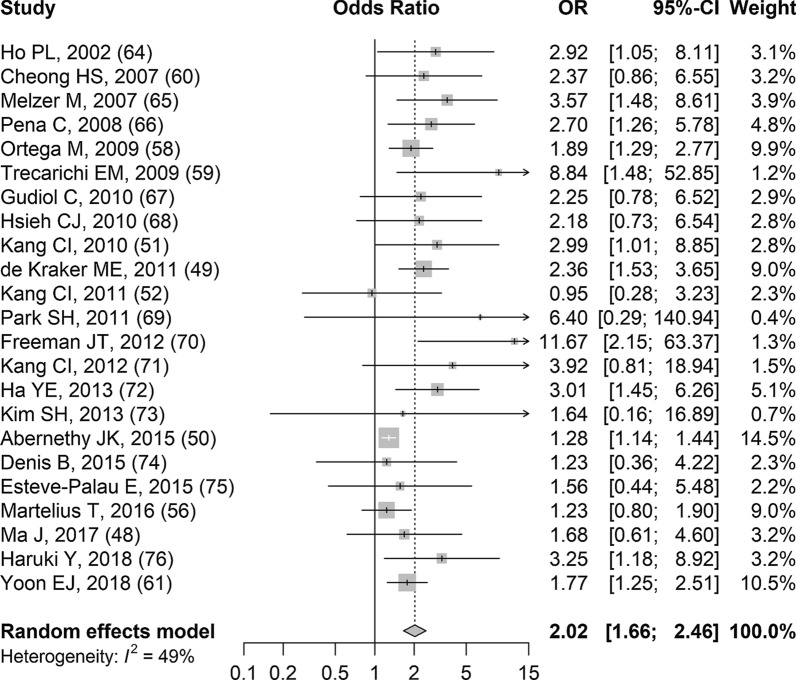
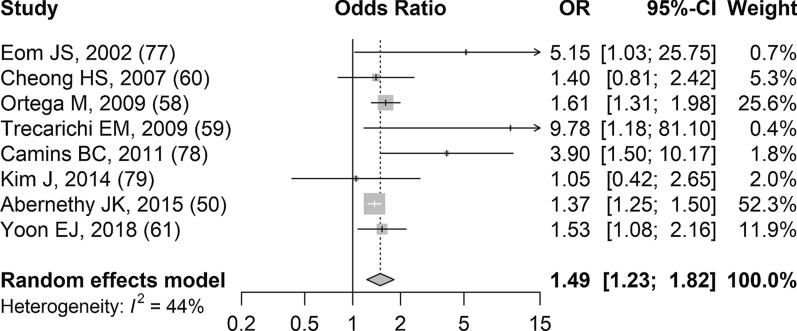
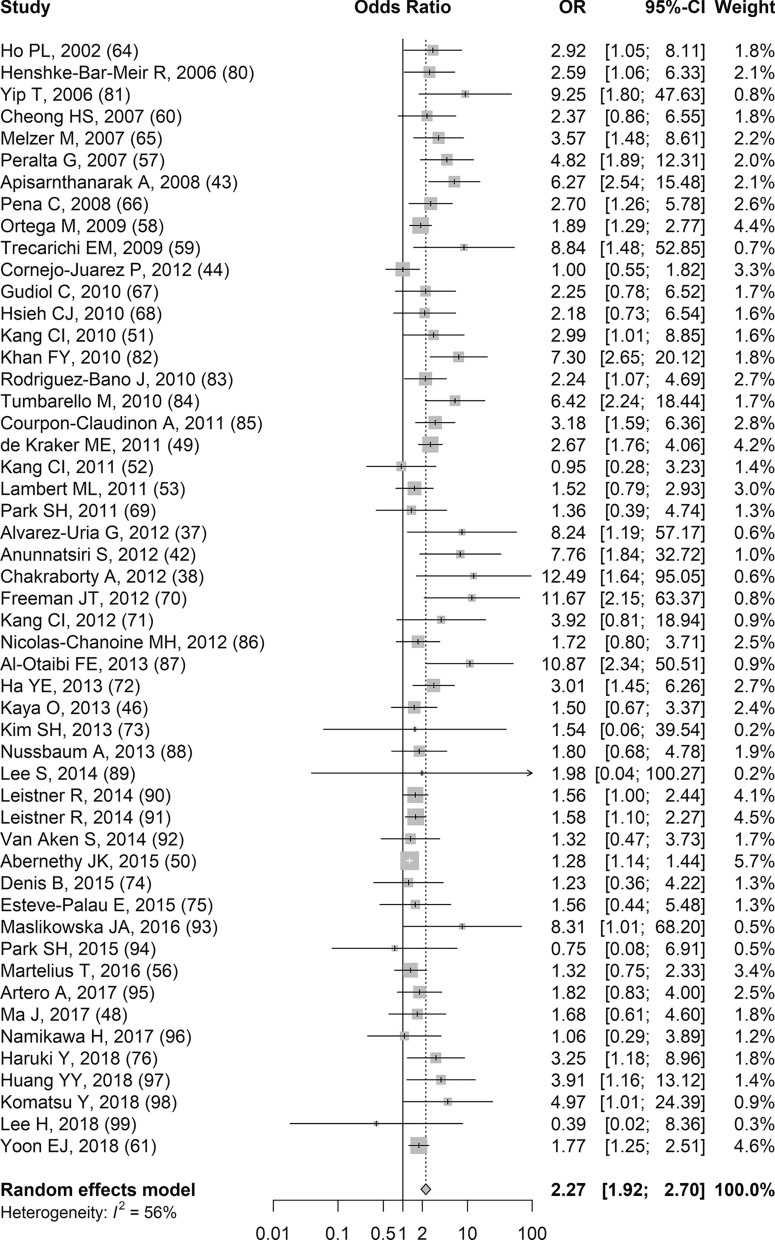
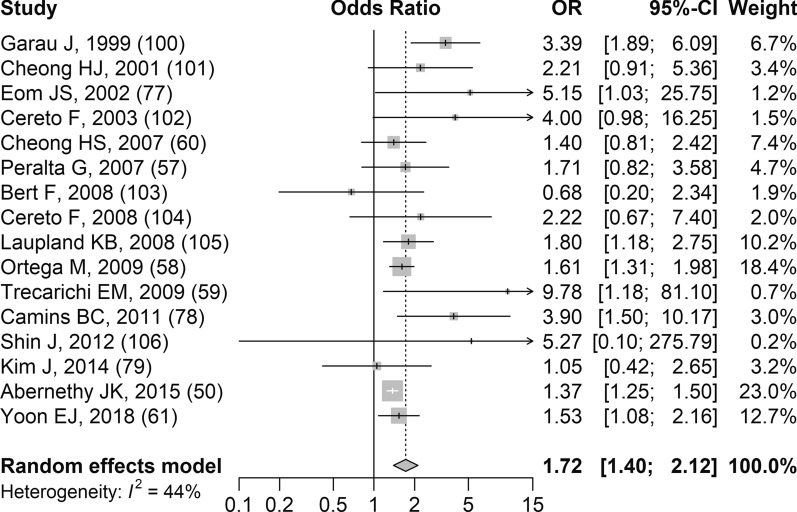
Results: Literature searches identified 14,759 de-duplicated records and 76 articles were included. Based on 30-day and all-cause mortality meta-analyses, regardless of the type of resistance, there was a significant increase in the odds of dying with resistant E. coli infections compared to susceptible infections. A summary mean difference was not presented for total length of hospital stay meta-analyses due to substantial to considerable heterogeneity. Since small numbers of studies contributed to meta-analyses for bacterium-attributable mortality and post-infection length of hospital stay, the summary results should be considered with caution. Studies contributing results for treatment failure and healthcare costs had considerable variability in definitions and reporting.
Conclusions: Overall, resistant E. coli infections were associated with significant 30-day and all-cause mortality burden. More research and/or improved reporting are necessary to facilitate quantitative syntheses of bacterium-attributable mortality, length of hospital stay, and hospital costs. Protocol Registration PROSPERO CRD42018111197.
Keywords: Antimicrobial resistance; Burden of disease; Escherichia coli; Length of hospital stay; Meta-analysis; Mortality; Multidrug resistance; Quinolone resistance; Systematic review; Third-generation cephalosporin resistance.
Conflict of interest statement
SAM: reports contracts from Health Canada, Public Health Agency of Canada and Ontario Ministry of Agriculture, Food and Rural Affairs, all outside the scope of the submitted work. All other authors declare that they have no competing interests.
Figures

References
-
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance. France 2014. https://apps.who.int/iris/bitstream/handle/10665/112642/9789241564748_en.... Accessed 21 Jan 2018.
-
- O’Neill J. Review on Antimicrobial Resistance. Antimicrobial Resistance: Tackling a crisis for the health and wealth of nations. 2014. https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Ta.... Accessed 29 Jun 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
