

Community use of face masks and similar barriers to prevent respiratory illness such as COVID-19: a rapid scoping review
- PMID: 33303066
- PMCID: PMC7730486
- DOI: 10.2807/1560-7917.ES.2020.25.49.2000725
Community use of face masks and similar barriers to prevent respiratory illness such as COVID-19: a rapid scoping review
Abstract
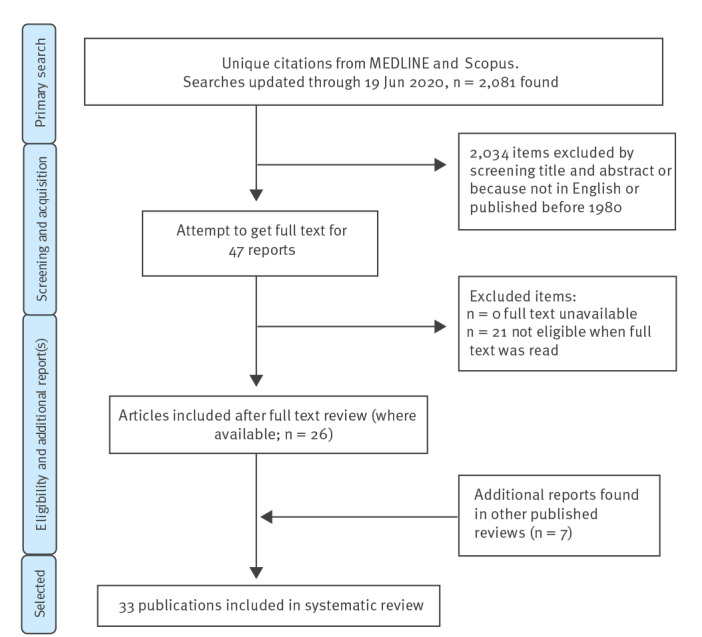
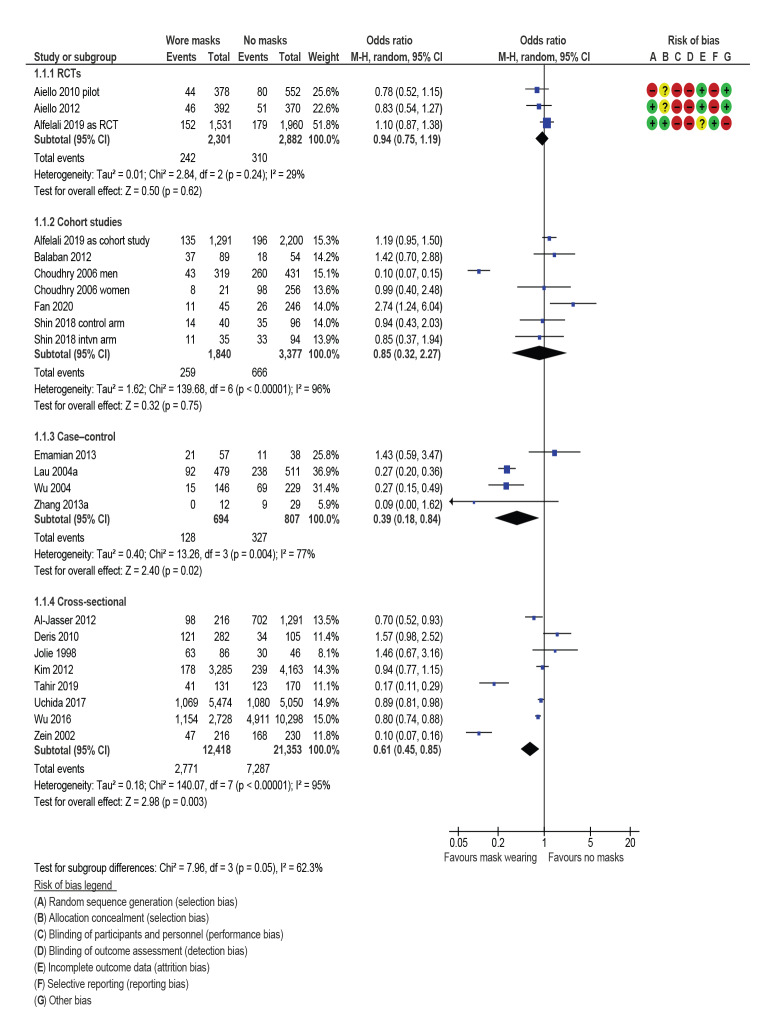
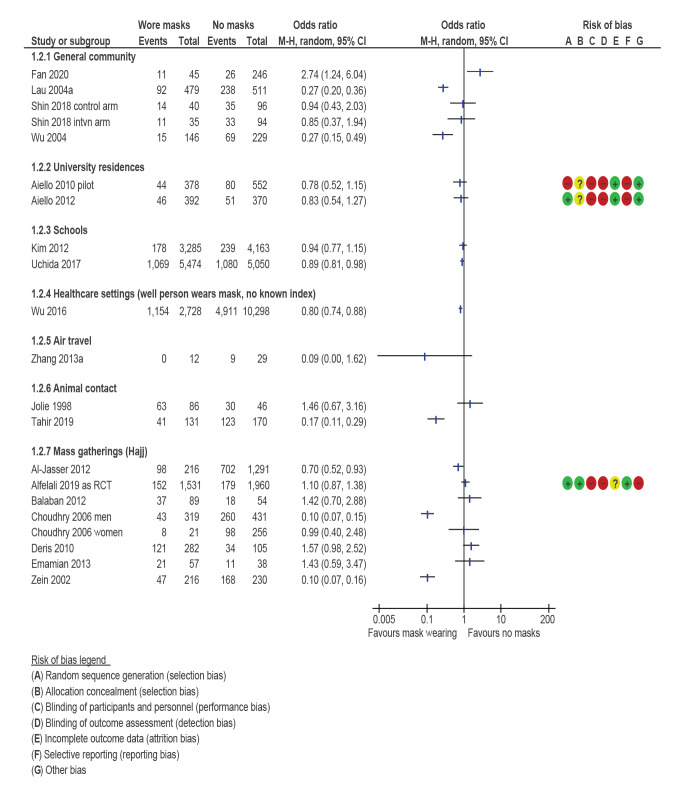
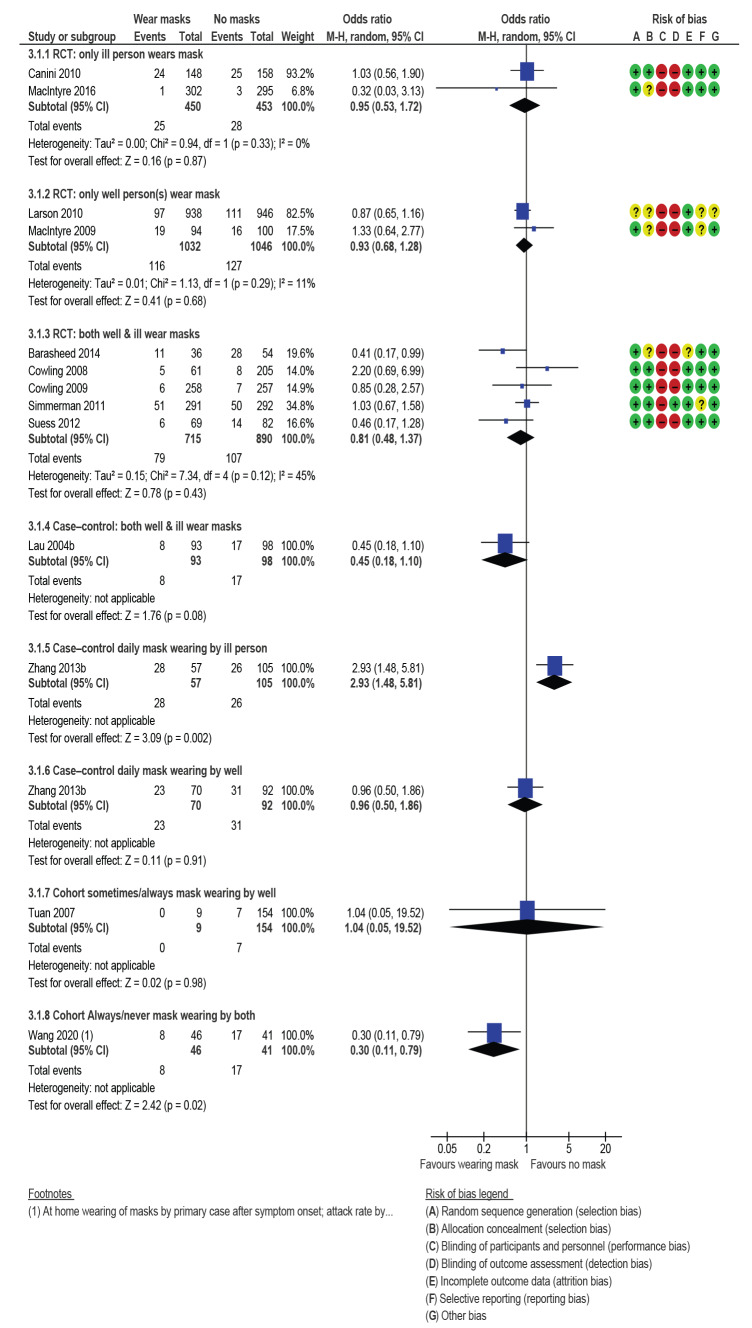
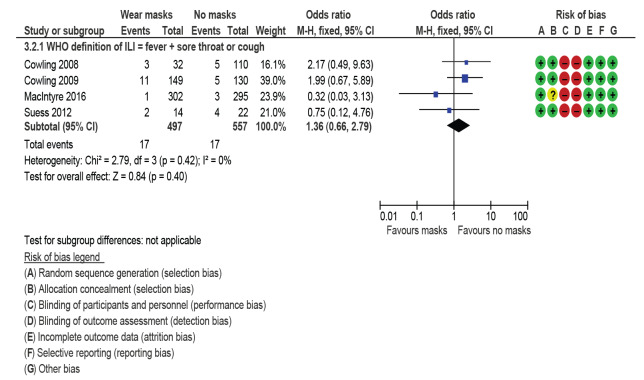
BackgroundEvidence for face-mask wearing in the community to protect against respiratory disease is unclear.AimTo assess effectiveness of wearing face masks in the community to prevent respiratory disease, and recommend improvements to this evidence base.MethodsWe systematically searched Scopus, Embase and MEDLINE for studies evaluating respiratory disease incidence after face-mask wearing (or not). Narrative synthesis and random-effects meta-analysis of attack rates for primary and secondary prevention were performed, subgrouped by design, setting, face barrier type, and who wore the mask. Preferred outcome was influenza-like illness. Grading of Recommendations, Assessment, Development and Evaluations (GRADE) quality assessment was undertaken and evidence base deficits described.Results33 studies (12 randomised control trials (RCTs)) were included. Mask wearing reduced primary infection by 6% (odds ratio (OR): 0.94; 95% CI: 0.75-1.19 for RCTs) to 61% (OR: 0.85; 95% CI: 0.32-2.27; OR: 0.39; 95% CI: 0.18-0.84 and OR: 0.61; 95% CI: 0.45-0.85 for cohort, case-control and cross-sectional studies respectively). RCTs suggested lowest secondary attack rates when both well and ill household members wore masks (OR: 0.81; 95% CI: 0.48-1.37). While RCTs might underestimate effects due to poor compliance and controls wearing masks, observational studies likely overestimate effects, as mask wearing might be associated with other risk-averse behaviours. GRADE was low or very low quality.ConclusionWearing face masks may reduce primary respiratory infection risk, probably by 6-15%. It is important to balance evidence from RCTs and observational studies when their conclusions widely differ and both are at risk of significant bias. COVID-19-specific studies are required.
Keywords: Hajj; coronavirus; face mask; influenza-like-illness; respiratory infection.
Conflict of interest statement
Figures

Comment in
-
Face masks and COVID-19: don't let perfect be the enemy of good.Euro Surveill. 2020 Dec;25(49):2001998. doi: 10.2807/1560-7917.ES.2020.25.49.2001998. Euro Surveill. 2020. PMID: 33303063 Free PMC article. No abstract available.
References
-
- World Health Organization (WHO). Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Geneva: WHO; 2020. Available from: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-... )
-
- World Health Organization (WHO). WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 March 2020. Geneva: WHO; 2020. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re...
-
- John Hopkins University Coronavirus Resource Centre. Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Baltimore: JHU; 2020. Available from: https://coronavirus.jhu.edu/map.html
-
- Gajanan M. Can Face Masks Prevent Coronavirus? Experts Say That Depends. Time. 2020 31 Jan.
-
- Asgari N, Wells P. Face mask shortage hits Europe and US as coronavirus spreads. Financial Times. 2020 30 Jan.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical