

Patent Foramen Ovale Attributable Cryptogenic Embolism With Thrombophilia Has Higher Risk for Recurrence and Responds to Closure
- PMID: 33303111
- PMCID: PMC9612803
- DOI: 10.1016/j.jcin.2020.09.059
Patent Foramen Ovale Attributable Cryptogenic Embolism With Thrombophilia Has Higher Risk for Recurrence and Responds to Closure
Abstract
Objectives: The aim of this study was to investigate the effect of management on the risk for recurrent events among patients with cryptogenic ischemic stroke or transient ischemic attack.
Background: The combination of patent foramen ovale (PFO) and hypercoagulability may greatly increase the risk for paradoxical embolism. However, previous randomized controlled trials evaluating the efficacy of PFO closure excluded these potential high-risk patients.
Methods: Patients diagnosed with PFO attributable cryptogenic embolism were prospectively, without randomization, recruited from January 2005 to March 2018. The relationship between thrombophilia and recurrent events was evaluated in overall patients. Multivariate Cox regression was conducted to assess the relative risk for recurrence in PFO closure and medical therapy groups.
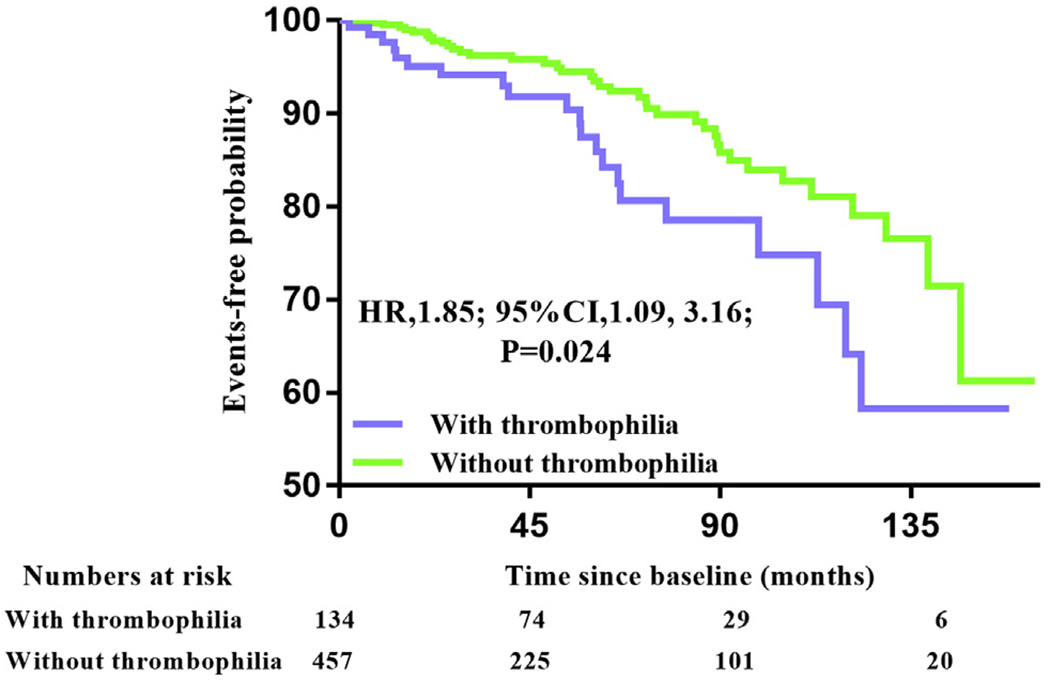
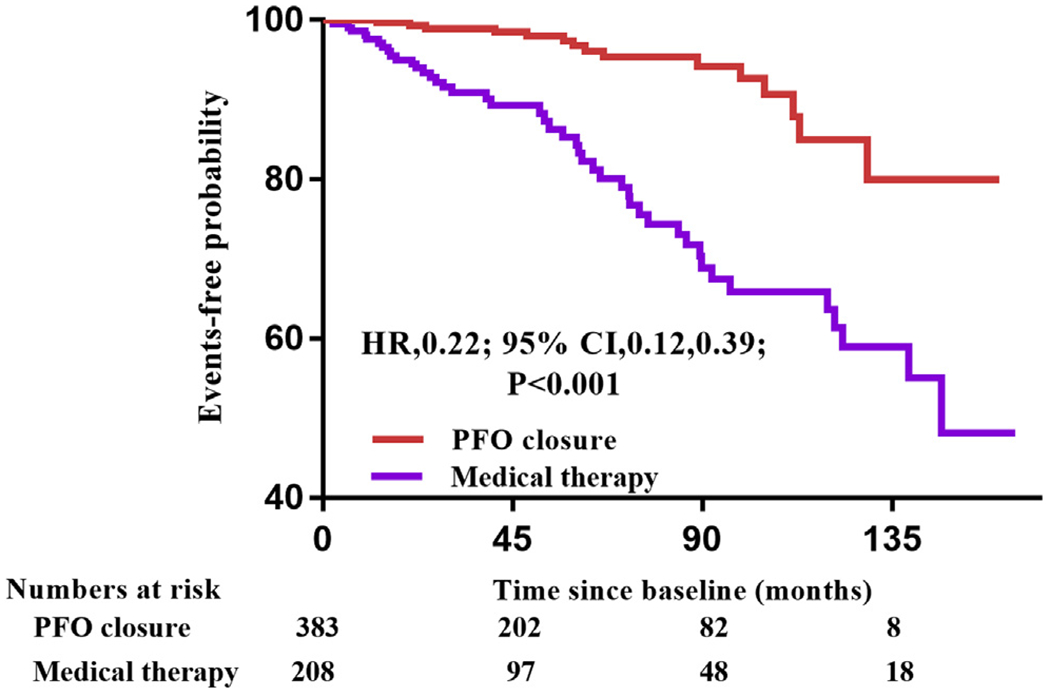
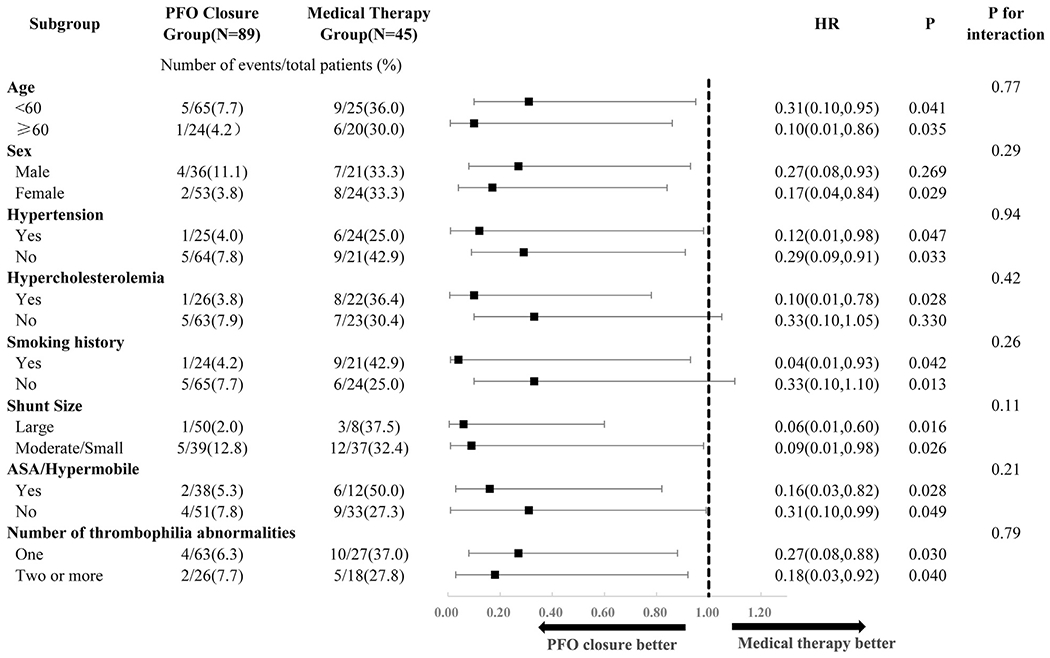
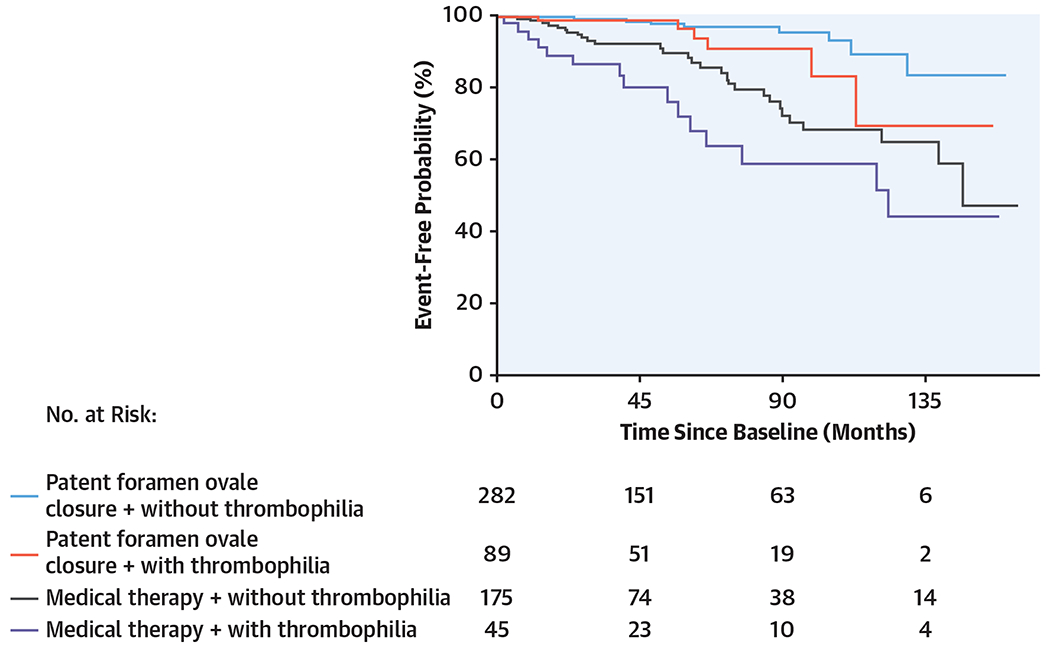
Results: A total of 591 patients with cryptogenic embolism with PFO were identified. The median duration of follow-up was 53 months, and thrombophilia significantly increased the risk for recurrent events (hazard ratio [HR]: 1.85; 95% confidence interval [CI]: 1.09 to 3.16; p = 0.024). PFO closure was superior to medical therapy in overall patients (HR: 0.16; 95% CI: 0.09 to 0.30; p < 0.001). Of the 134 patients (22.7%) with thrombophilia, there was a difference in the risk for recurrence events between the PFO closure (6 of 89) and medical therapy (15 of 45) groups (HR: 0.25; 95% CI: 0.08 to 0.74; p = 0.012). There was no potential heterogeneity in the further subgroup analysis.
Conclusions: Patients with cryptogenic stroke with PFO and hypercoagulable state had increased risk for recurrent stroke or transient ischemic attack. PFO closure provided a lower risk for recurrent events compared with medical therapy alone.
Keywords: closure; cryptogenic stroke; patent foramen ovale; secondary prevention; thrombophilia.
Copyright © 2020. Published by Elsevier Inc.
Conflict of interest statement
Author Disclosures This study was funded by the National Institutes of Health (grant NS051588 to Dr. Ning). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Patent Foramen Ovale: Closing the Gap of Indications for Closure-Time for a Patient-Tailored Therapy.JACC Cardiovasc Interv. 2020 Dec 14;13(23):2753-2754. doi: 10.1016/j.jcin.2020.10.038. JACC Cardiovasc Interv. 2020. PMID: 33303112 No abstract available.
-
Reply: Shouldn't Patients With Paradoxical Emboli and Thrombophilia Be Given Anticoagulant Agents?JACC Cardiovasc Interv. 2021 Mar 8;14(5):583-584. doi: 10.1016/j.jcin.2021.01.002. Epub 2021 Mar 1. JACC Cardiovasc Interv. 2021. PMID: 33663787 No abstract available.
-
Shouldn't Patients With Paradoxical Emboli and Thrombophilia Be Given Anticoagulant Agents?JACC Cardiovasc Interv. 2021 Mar 8;14(5):583. doi: 10.1016/j.jcin.2020.12.024. Epub 2021 Mar 1. JACC Cardiovasc Interv. 2021. PMID: 33663788 No abstract available.
References
-
- Lijfering WM, Brouwer JL, Veeger NJ, et al. Selective testing for thrombophilia in patients with first venous thrombosis: results from a retrospective family cohort study on absolute thrombotic risk for currently known thrombophilic defects in 2479 relatives. Blood 2009;113: 5314–22. - PubMed
-
- Vossen CY, Walker ID, Svensson P, et al. Recurrence rate after a first venous thrombosis in patients with familial thrombophilia. Arterioscler Thromb Vasc Biol 2005;25:1992–7. - PubMed
-
- Kenet G, Lutkhoff LK, Albisetti M, et al. Impact of thrombophilia on risk of arterial ischemic stroke or cerebral sinovenous thrombosis in neonates and children: a systematic review and meta-analysis of observational studies. Circulation 2010;121:1838–47. - PubMed
-
- Carod-Artal FJ, Nunes SV, Portugal D, Silva TV, Vargas AP. Ischemic stroke subtypes and thrombophilia in young and elderly Brazilian stroke patients admitted to a rehabilitation hospital. Stroke 2005;36:2012–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
