

Safety and feasibility evaluation of planning and execution of surgical revascularisation solely based on coronary CTA and FFRCT in patients with complex coronary artery disease: study protocol of the FASTTRACK CABG study
- PMID: 33303435
- PMCID: PMC7733219
- DOI: 10.1136/bmjopen-2020-038152
Safety and feasibility evaluation of planning and execution of surgical revascularisation solely based on coronary CTA and FFRCT in patients with complex coronary artery disease: study protocol of the FASTTRACK CABG study
Abstract
Introduction: The previously published SYNTAX III REVOLUTION trial demonstrated that clinical decision-making between coronary artery bypass graft (CABG) and percutaneous coronary intervention based on coronary CT angiography (CCTA) had a very high agreement with the treatment decision derived from invasive coronary angiography (ICA). The study objective of the FASTTRACK CABG is to assess the feasibility of CCTA and fractional flow reserve derived from CTA (FFRCT) to replace ICA as a surgical guidance method for planning and execution of CABG in patients with three-vessel disease with or without left main disease.
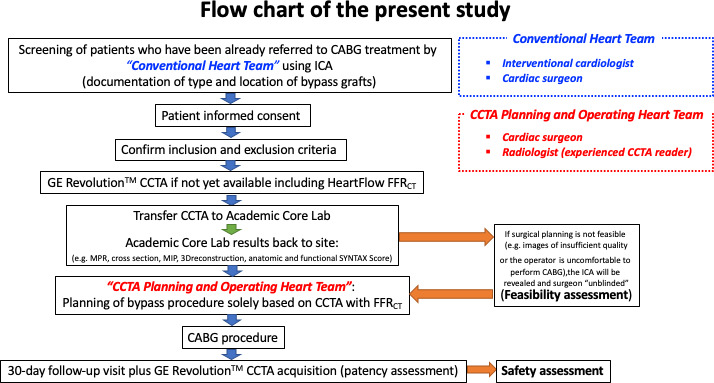
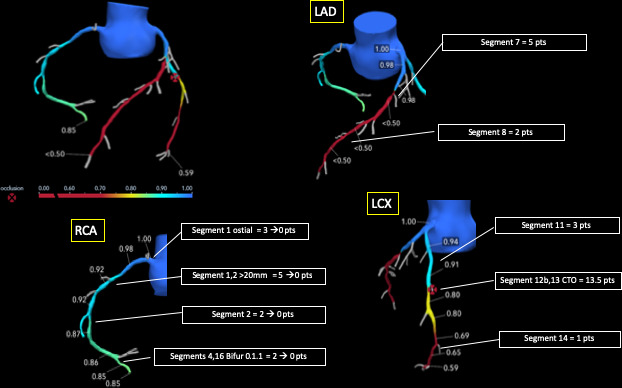
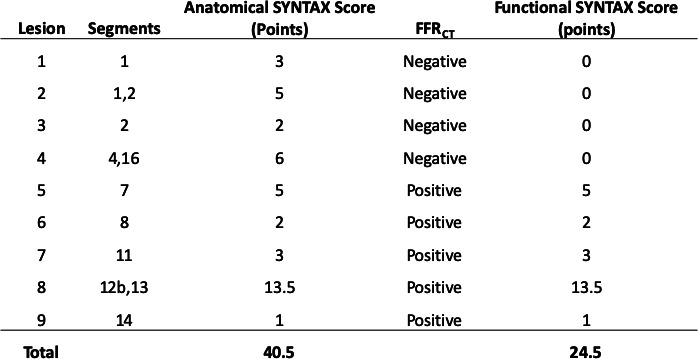
Methods and analysis: The FASTTRACK CABG is an investigator-initiated single-arm, multicentre, prospective, proof-of-concept and first-in-man study with feasibility and safety analysis. Surgical revascularisation strategy and treatment planning will be solely based on CCTA and FFRCT without knowledge of the anatomy defined by ICA. Clinical follow-up visit including CCTA will be performed 30 days after CABG in order to assess graft patency and adequacy of the revascularisation with respect to the surgical planning based on non-invasive imaging (CCTA) with functional assessment (FFRCT) and compared with ICA. Primary feasibility endpoint is CABG planning and execution solely based on CCTA and FFRCT in 114 patients. Primary safety endpoint based on 30 day CCTA is graft assessment and topographical adequacy of the revascularisation procedure. Automatic non-invasive assessment of functional coronary anatomy complexity is also evaluated with FFRCT for functional Synergy Between percutaneous coronary intervention With Taxus and Cardiac Surgery Score assessment on CCTA. CCTA with FFRCT might provide better anatomical and functional analysis of the coronary circulation leading to appropriate anatomical and functional revascularisation, and thereby contributing to a better outcome.
Ethics and dissemination: Each patient has to provide written informed consent as approved by the ethical committee of the respective clinical site. Results will be submitted for publication in peer-reviewed journals and will be disseminated at scientific conferences.
Trial registration number: NCT04142021.
Keywords: cardiac surgery; cardiology; cardiothoracic surgery; cardiovascular imaging; coronary heart disease; ischaemic heart disease.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GWS reports personal fees from Terumo, personal fees from Amaranth, personal fees from Shockwave, personal fees from Valfix, personal fees from TherOx, personal fees from Reva, personal fees from Vascular Dynamics, personal fees from Robocath, personal fees from HeartFlow, personal fees from Gore, personal fees from Ablative Solutions, personal fees from Matrizyme, personal fees from Miracor, personal fees from Neovasc, personal fees from V-wave, personal fees from Abiomed, personal fees from Claret, personal fees from Sirtex, personal fees and other from Ancora, personal fees and other from Qool Therapeutics, other from Cagent, other from Applied Therapeutics, other from Biostar family of funds, other from MedFocus family of funds, personal fees and other from SpectraWave, personal fees from MAIA Pharmaceuticals, personal fees and other from Orchestra Biomed, other from Aria, outside the submitted work. JL is a consultant to and holds stock options in HeartFlow and Circle CVI and receives research grant support from GE Healthcare. BT is an employee of GE Healthcare. CT and CR report personal fees from HeartFlow, Inc, during the conduct of the study. PWS reports personal fees from Biosensors, Medtronic, Micel Technologies, Sinomedical Sciences Technology, St. Jude Medical, Philips/Volcano, Xeltis, and HeartFlow, outside the submitted work. All other authors have no conflict of interest to declare.
Figures
References
-
- Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet 2013;381:639–50. 10.1016/S0140-6736(13)60108-7 - DOI - PubMed
-
- Sianos G, Morel M-A, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention 2005;1:219–27. - PubMed
-
- Serruys PW, Chichareon P, Modolo R, et al. The SYNTAX score on its way out or…towards artificial intelligence: Part I. EuroIntervention 2019.
-
- Serruys PW, Chichareon P, Modolo R, et al. The SYNTAX score on its way out or…towards artificial intelligence: Part II. EuroIntervention 2019.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous