

Effects of Dexmedetomidine on Emergence Agitation and Recovery Quality Among Children Undergoing Surgery Under General Anesthesia: A Meta-Analysis of Randomized Controlled Trials
- PMID: 33304867
- PMCID: PMC7694572
- DOI: 10.3389/fped.2020.580226
Effects of Dexmedetomidine on Emergence Agitation and Recovery Quality Among Children Undergoing Surgery Under General Anesthesia: A Meta-Analysis of Randomized Controlled Trials
Abstract
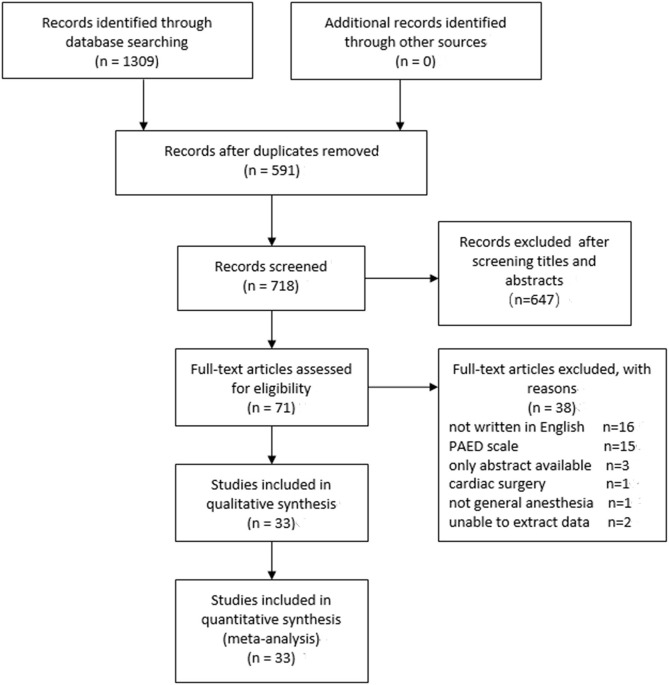
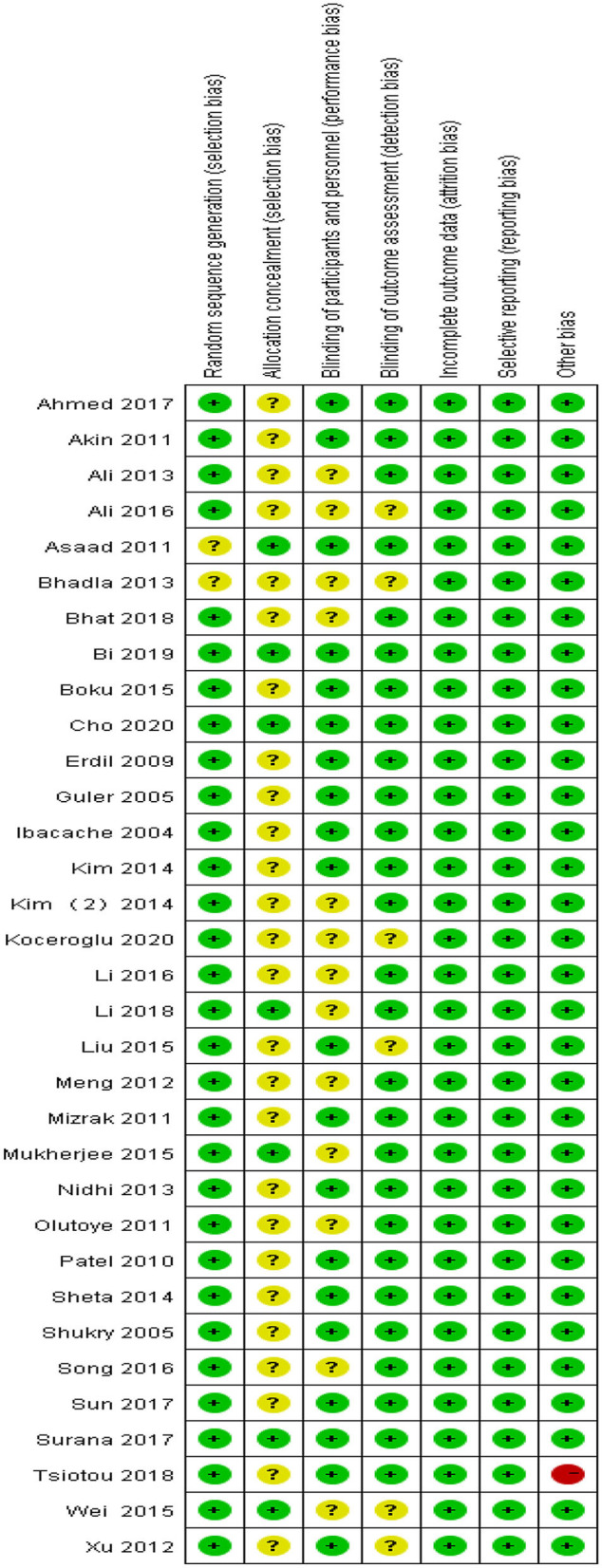
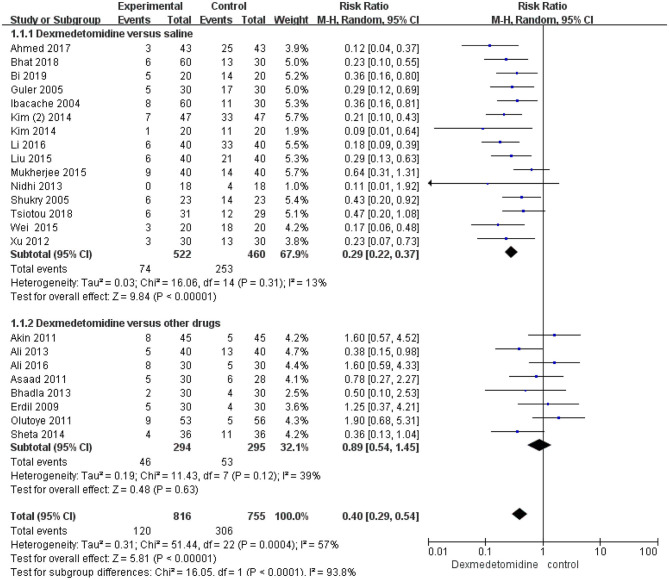
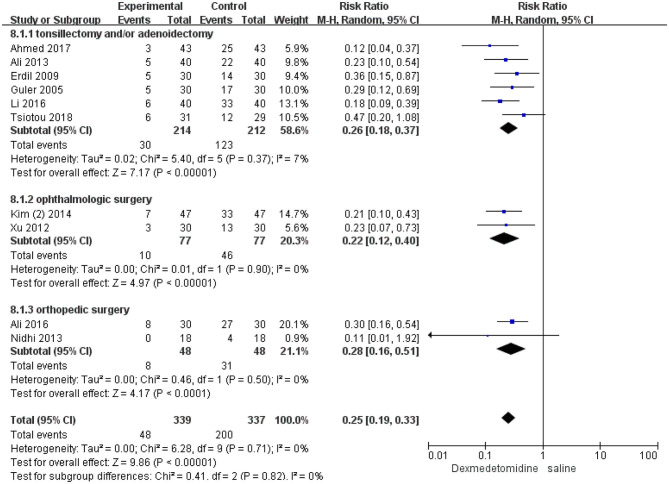
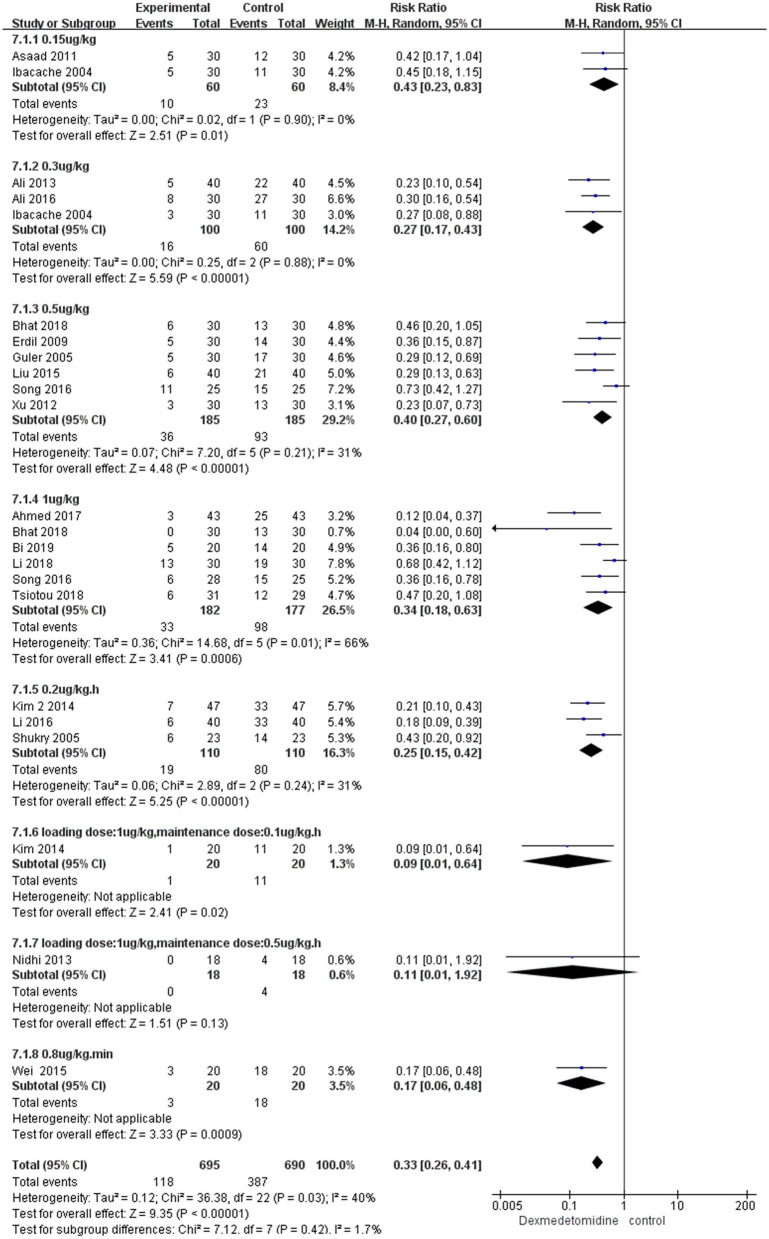
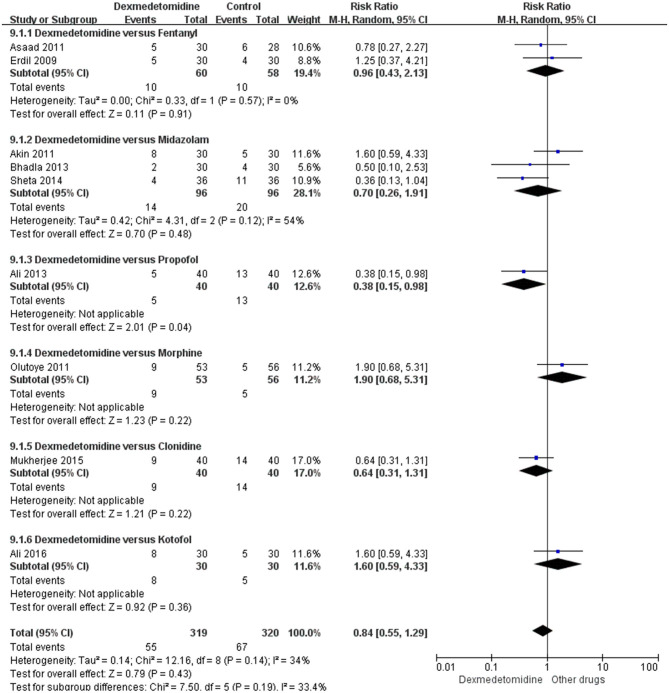
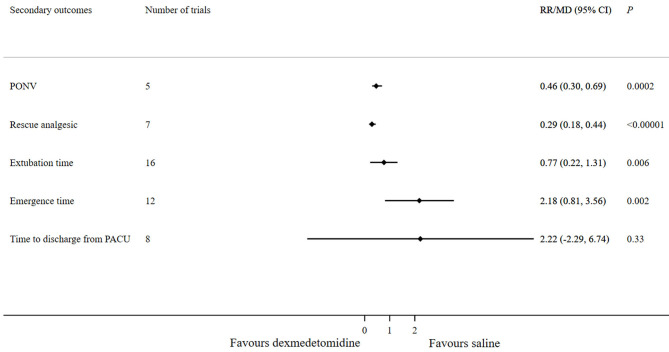
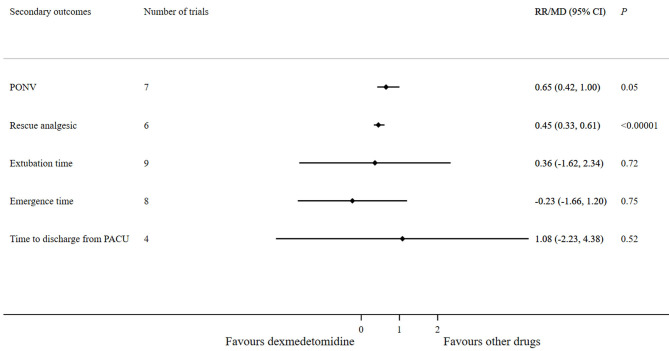
Background: Emergence agitation (EA) is one of the most common and intractable postoperative complications among children undergoing surgery under general anesthesia. Dexmedetomidine, an α(2)-adrenoceptor agonist, offers an ideal sedation, reduces preoperative anxiety, and facilitates smooth induction of anesthesia, and it is widely used in pediatric surgery. We aimed to evaluate the efficacy of dexmedetomidine for preventing emergence agitation in children after general anesthesia. Methods: We comprehensively reviewed PubMed, Cochrane Library, EMBASE, and Web of Science databases to search all randomized controlled trials, published before April 22, 2020, investigating the efficacy of dexmedetomidine in preventing the emergence agitation in children after general anesthesia. The meta-analysis was performed using Review Manager 5.3. The primary outcome was the incidence of emergence agitation. Secondary outcomes included the number of patients requiring rescue analgesic, number of patients with postoperative nausea and vomiting, emergence time, extubation time, and time to discharge from the post-anesthesia care unit. Results: We included a total of 33 studies, comprising 2,549 patients in this meta-analysis. Compared with saline, dexmedetomidine significantly reduced the emergence agitation incidence [risk ratio (RR) 0.29; 95% confidence interval (CI) 0.22-0.37; p < 0.00001], incidence of postoperative nausea and vomiting (RR 0.46; 95% CI 0.3-0.69; p = 0.0002), and the requirement of rescue analgesic (RR 0.29; 95% CI 0.18-0.44; p < 0.00001). Furthermore, children in the dexmedetomidine group experienced a longer emergence time [mean difference (MD) 2.18; 95% CI 0.81-3.56; p = 0.002] and extubation time (MD 0.77; 95% CI 0.22-1.31; p = 0.006) compared with those in the saline group. However, no significant difference was observed in the time to discharge from the post-anesthesia care unit (MD 2.22; 95% CI -2.29-6.74; p = 0.33) between the two groups. No significant differences were observed between the effects of dexmedetomidine and other drugs like midazolam, propofol, fentanyl, tramadol, and clonidine in terms of the emergence agitation incidence and other parameters, except for the requirement of rescue analgesic (RR 0.45; 95% CI 0.33-0.61; p < 0.00001). Conclusions: Dexmedetomidine can prevent emergence agitation, relieves postoperative pain, decreases the requirement of rescue analgesic, and decreases the postoperative nausea and vomiting events.
Keywords: children; dexmedetomidine; emergence agitation; general anesthesia; meta-analysis.
Copyright © 2020 Yang, Hu, Peng, Chen, Zhou, Yang, Yang and Wang.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous