

HIV-Associated CKDs in Children and Adolescents
- PMID: 33305123
- PMCID: PMC7710839
- DOI: 10.1016/j.ekir.2020.09.001
HIV-Associated CKDs in Children and Adolescents
Abstract
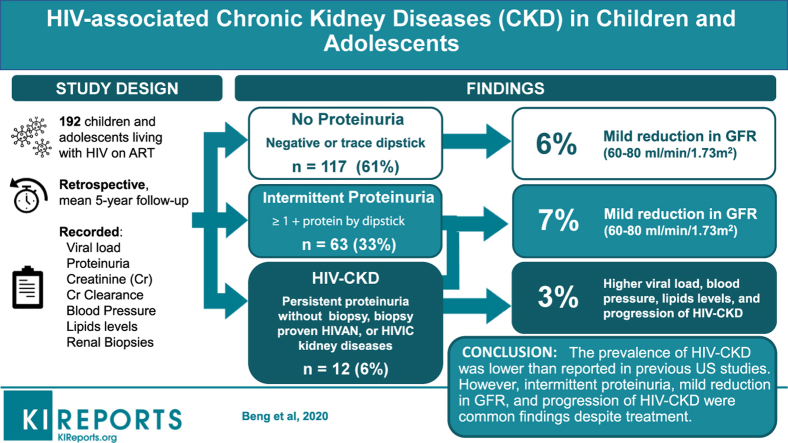
Introduction: Limited information is available describing the current prevalence of proteinuria and HIV-associated CKDs (HIV-CKDs) in children and adolescents living with HIV and receiving antiretroviral therapy in the United States.
Methods: To address this issue, we performed a retrospective study of children and adolescents living with HIV who received medical care at Children's National Hospital in Washington, DC, between January 2012 and July 2019. Demographic data, clinical parameters (mode of HIV transmission, viral loads, CD4 cell counts, serum creatinine, glomerular filtration rate [GFR], plasma lipid levels, proteinuria, blood pressure, renal biopsies), and medical treatments, all done as a standard of clinical care, were collected and analyzed.
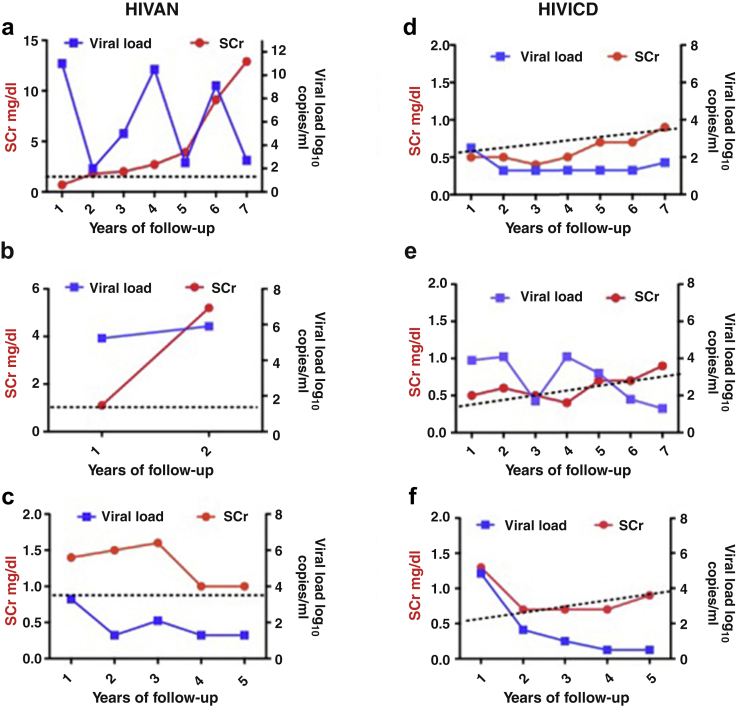
Results: The majority of the 192 patients enrolled were of African descent (88%) and acquired HIV through vertical transmission (97%). The prevalence of all HIV-CKDs was 6%. Of these patients, 39% had intermittent or persistent proteinuria, and 7% percent had proteinuria with a mild decline in GFR (60-80 ml/min per 1.73 m2), and 6% had a mild decline in GFR without proteinuria. Documented hypertension was present in 6% of the patients, mainly in association with HIV-CKD. Patients with persistent proteinuria (3%) and biopsy-proven HIV-CKD had a slow but constant progression of their renal diseases.
Conclusions: The prevalence of persistent proteinuria and HIV-CKD was lower than that reported in previous studies conducted in the United States. However, intermittent proteinuria, mild reductions in GFR, and progression of established HIV-CKD were common findings in this group of patients with predominantly vertically acquired HIV who were receiving antiretroviral therapy.
Keywords: HIV-associated nephropathy; adolescents; children; kidney diseases; proteinuria.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures


References
-
- Strauss J., Abitbol C., Zilleruelo G. Renal disease in children with the acquired immunodeficiency syndrome. N Engl J Med. 1989;321:625–630. - PubMed
-
- Ray P.E., Rakusan T., Loechelt B.J. Human immunodeficiency virus (HIV)-associated nephropathy in children from the Washington, D.C. area: 12 years’ experience. Semin Nephrol. 1998;18:396–405. - PubMed
-
- Chaparro A.I., Mitchell C.D., Abitbol C.L. Proteinuria in children infected with the human immunodeficiency virus. J Pediatr. 2008;152(6):844–849. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
