

COVID-19 vaccine hesitancy in the UK: the Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II
- PMID: 33305716
- PMCID: PMC7804077
- DOI: 10.1017/S0033291720005188
COVID-19 vaccine hesitancy in the UK: the Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II
Abstract
Background: Our aim was to estimate provisional willingness to receive a coronavirus 2019 (COVID-19) vaccine, identify predictive socio-demographic factors, and, principally, determine potential causes in order to guide information provision.
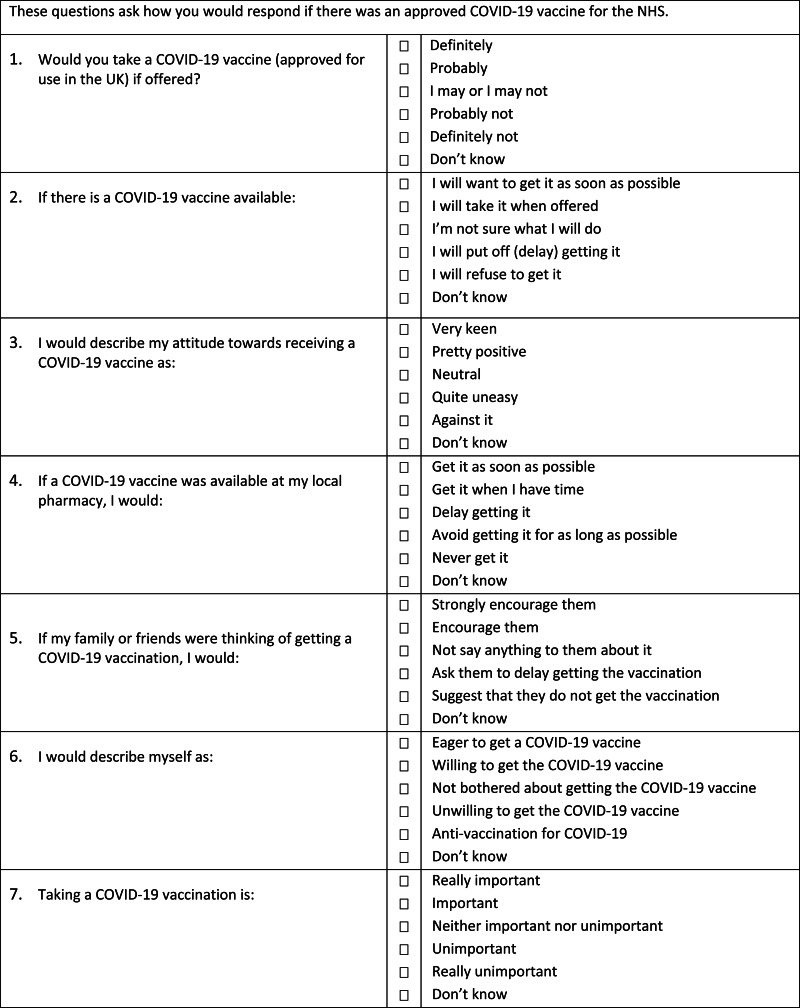
Methods: A non-probability online survey was conducted (24th September-17th October 2020) with 5,114 UK adults, quota sampled to match the population for age, gender, ethnicity, income, and region. The Oxford COVID-19 vaccine hesitancy scale assessed intent to take an approved vaccine. Structural equation modelling estimated explanatory factor relationships.
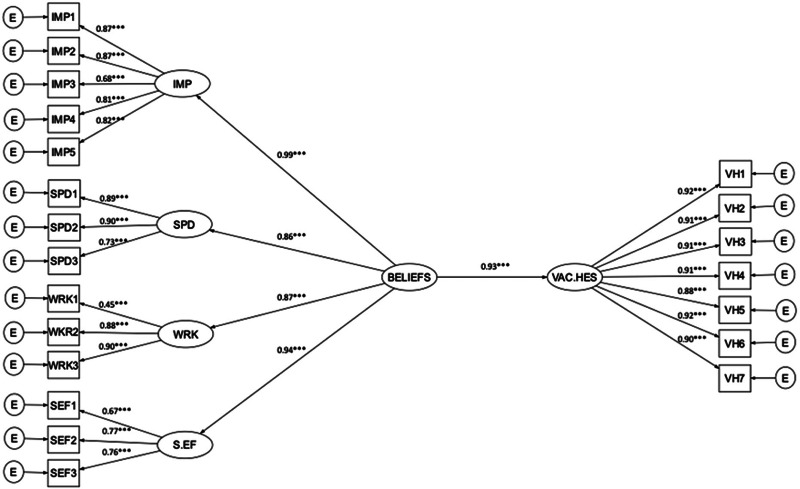
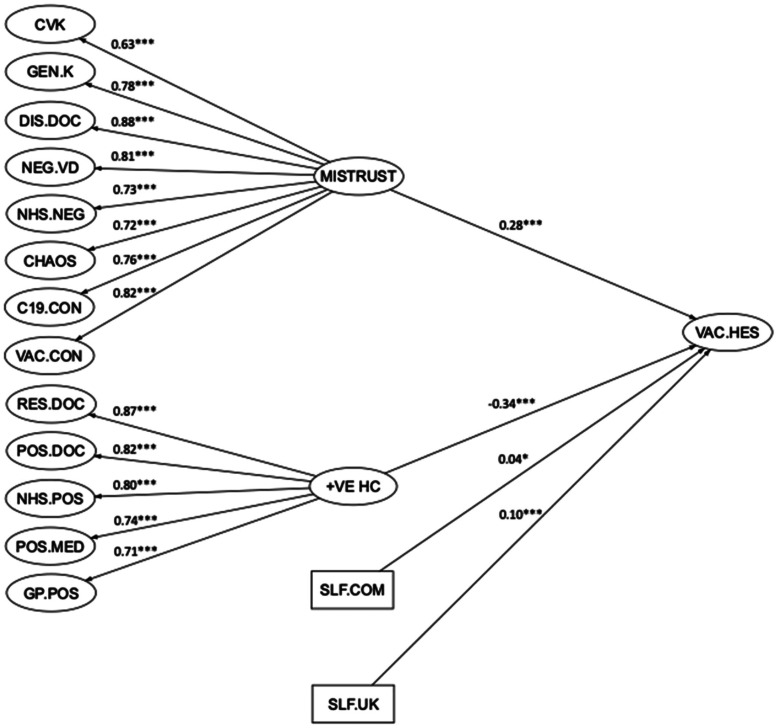
Results: 71.7% (n=3,667) were willing to be vaccinated, 16.6% (n=849) were very unsure, and 11.7% (n=598) were strongly hesitant. An excellent model fit (RMSEA=0.05/CFI=0.97/TLI=0.97), explaining 86% of variance in hesitancy, was provided by beliefs about the collective importance, efficacy, side-effects, and speed of development of a COVID-19 vaccine. A second model, with reasonable fit (RMSEA=0.03/CFI=0.93/TLI=0.92), explaining 32% of variance, highlighted two higher-order explanatory factors: 'excessive mistrust' (r=0.51), including conspiracy beliefs, negative views of doctors, and need for chaos, and 'positive healthcare experiences' (r=-0.48), including supportive doctor interactions and good NHS care. Hesitancy was associated with younger age, female gender, lower income, and ethnicity, but socio-demographic information explained little variance (9.8%). Hesitancy was associated with lower adherence to social distancing guidelines.
Conclusions: COVID-19 vaccine hesitancy is relatively evenly spread across the population. Willingness to take a vaccine is closely bound to recognition of the collective importance. Vaccine public information that highlights prosocial benefits may be especially effective. Factors such as conspiracy beliefs that foster mistrust and erode social cohesion will lower vaccine up-take.
Keywords: Covid-19 vaccine hesitancy; conspiracy beliefs; mistrust; vaccine confidence.
Figures
References
-
- Adler, N. E., Epel, E. S., Castellazzo, G., & Ickovics, J. R. (2000). Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychology, 19(6), 586–592. - PubMed
-
- Akkerman, A., Mudde, C., & Zaslove, A. (2014) How populist are the people? Measuring populist attitudes in voters. Comparative Political Studies, 47, 1324–1353.
-
- Bedford, H., Attwell, K., Danchin, M., Marshall, H. Corben, P., & Leask, J. (2018). Vaccine hesitancy, refusal and access barriers: The need for clarity in terminology. Vaccine, 36, 6556–6558. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
