

The relationship between excessive dietary fructose consumption and paediatric fatty liver disease
- PMID: 33305889
- PMCID: PMC8195317
- DOI: 10.1111/ijpo.12759
The relationship between excessive dietary fructose consumption and paediatric fatty liver disease
Abstract
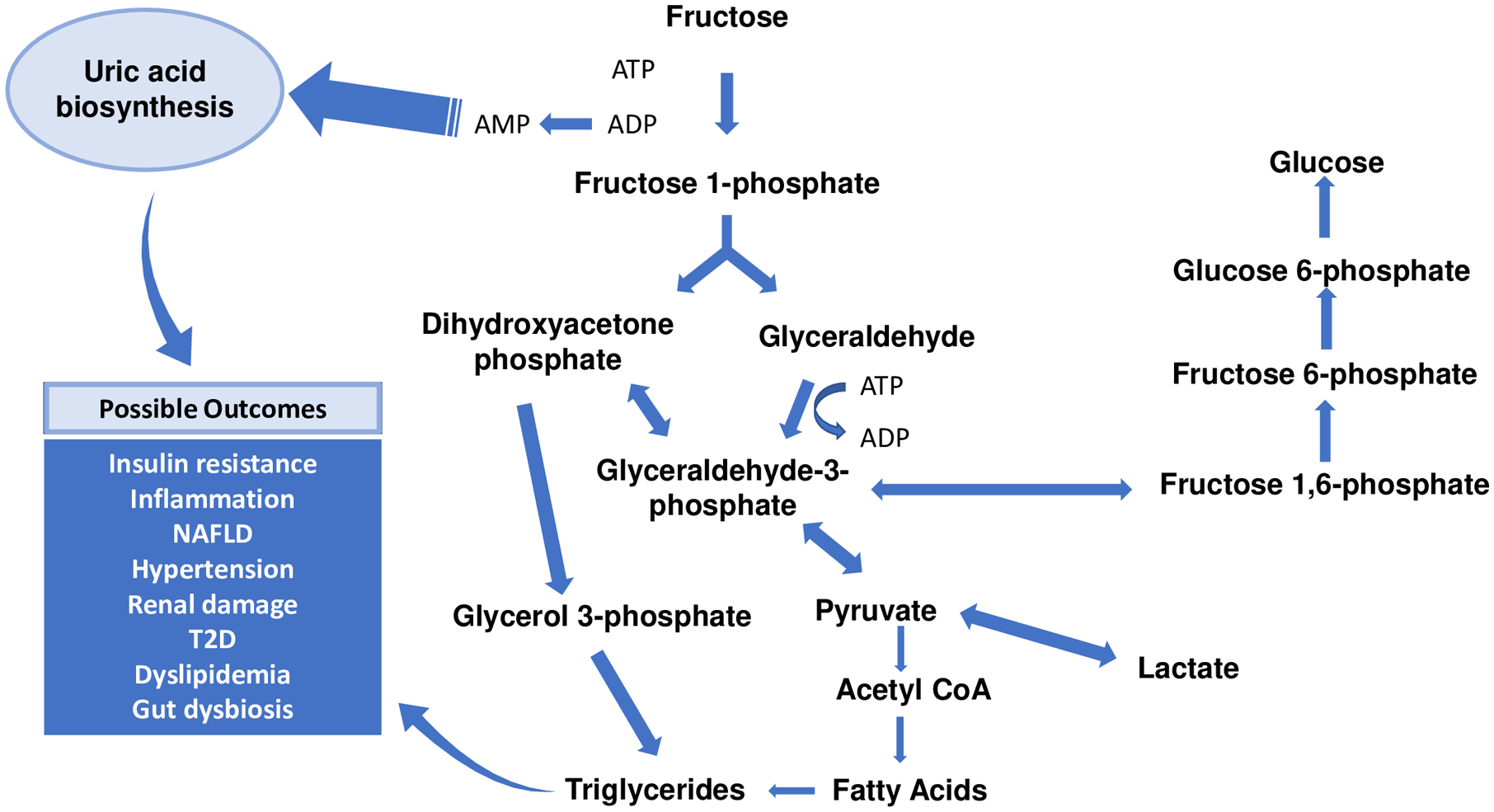
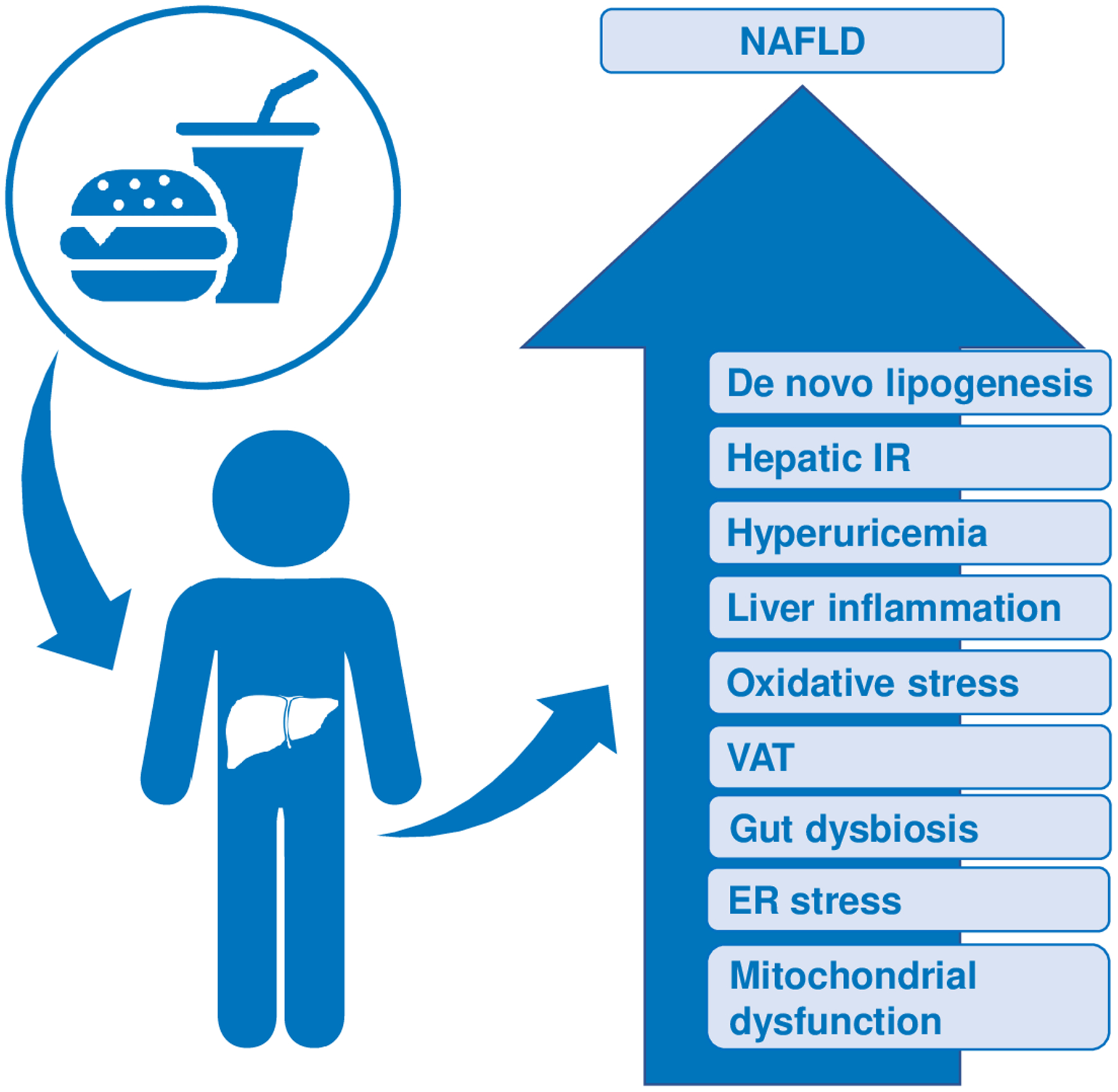
The global prevalence of non-alcoholic fatty liver disease (NAFLD) in children and adolescents is escalating and currently represents the most common chronic liver disease in the paediatric population. NAFLD is associated with high daily caloric intake and sedentary behaviour, with excessive consumption of added sugar emerging as an important contributor to NAFLD risk in children. This is a particularly important factor for adolescents with obesity, who are the heaviest consumers of added sugar. Table sugar, or sucrose, is a disaccharide comprised of fructose and glucose, yet only fructose has been strongly linked to NAFLD pathogenesis largely due to the unique characteristics of its metabolism and detrimental effects on key metabolic pathways. To date, the relationship between excessive fructose intake and risk of NAFLD in children and adolescents remains incompletely understood, and it is not yet known whether fructose actually causes NAFLD or instead exacerbates hepatic fat accumulation and possible hepatocellular injury only within the context of cardiometabolic factors. The purpose of this review is to summarize recent studies linking fructose consumption with NAFLD in the paediatric population and integrate results from interventional studies of fructose restriction in children and adolescents on NAFLD and related metabolic markers. Given the overall positive impact of lifestyle modifications in the management of paediatric NAFLD, reduction of added sugar consumption may represent an important, early opportunity to mitigate or prevent NAFLD in high-risk children and adolescents.
Keywords: fructose; hepatic steatosis; liver fibrosis; non-alcoholic fatty liver disease; non-alcoholic steatohepatitis; uric acid.
© 2020 World Obesity Federation.
Figures
References
-
- Vos MB, Abrams SH, Barlow SE, et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). J Pediatr Gastroenterol Nutr. February 2017;64(2):319–334. doi: 10.1097/MPG.0000000000001482 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
