

Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19
- PMID: 33306283
- PMCID: PMC7745180
- DOI: 10.1056/NEJMoa2031994
Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19
Abstract
Background: Severe coronavirus disease 2019 (Covid-19) is associated with dysregulated inflammation. The effects of combination treatment with baricitinib, a Janus kinase inhibitor, plus remdesivir are not known.
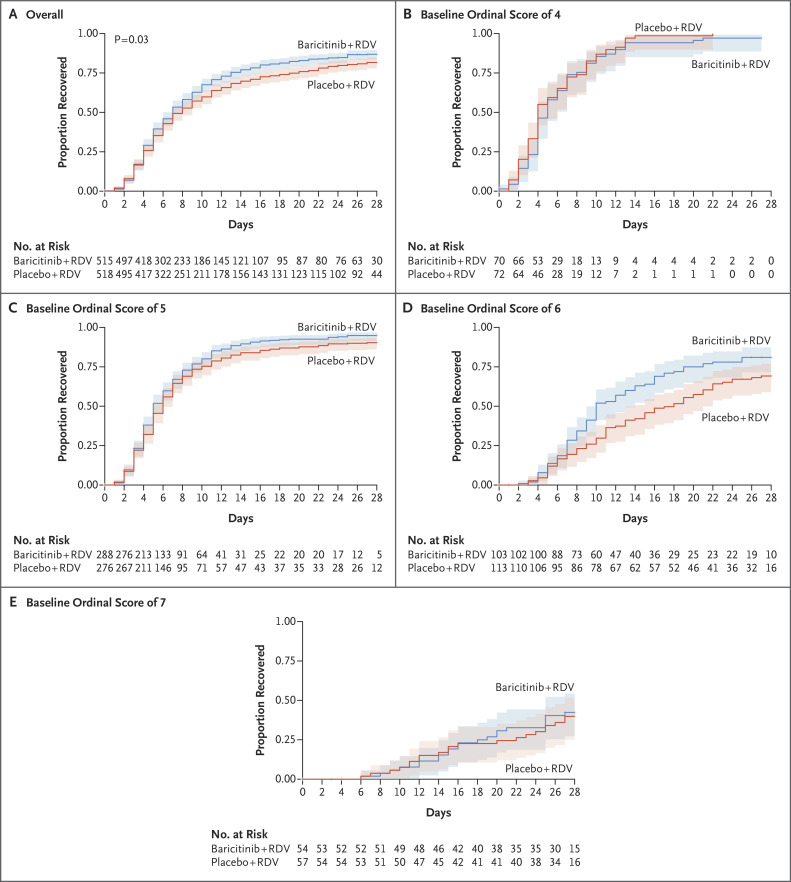
Methods: We conducted a double-blind, randomized, placebo-controlled trial evaluating baricitinib plus remdesivir in hospitalized adults with Covid-19. All the patients received remdesivir (≤10 days) and either baricitinib (≤14 days) or placebo (control). The primary outcome was the time to recovery. The key secondary outcome was clinical status at day 15.
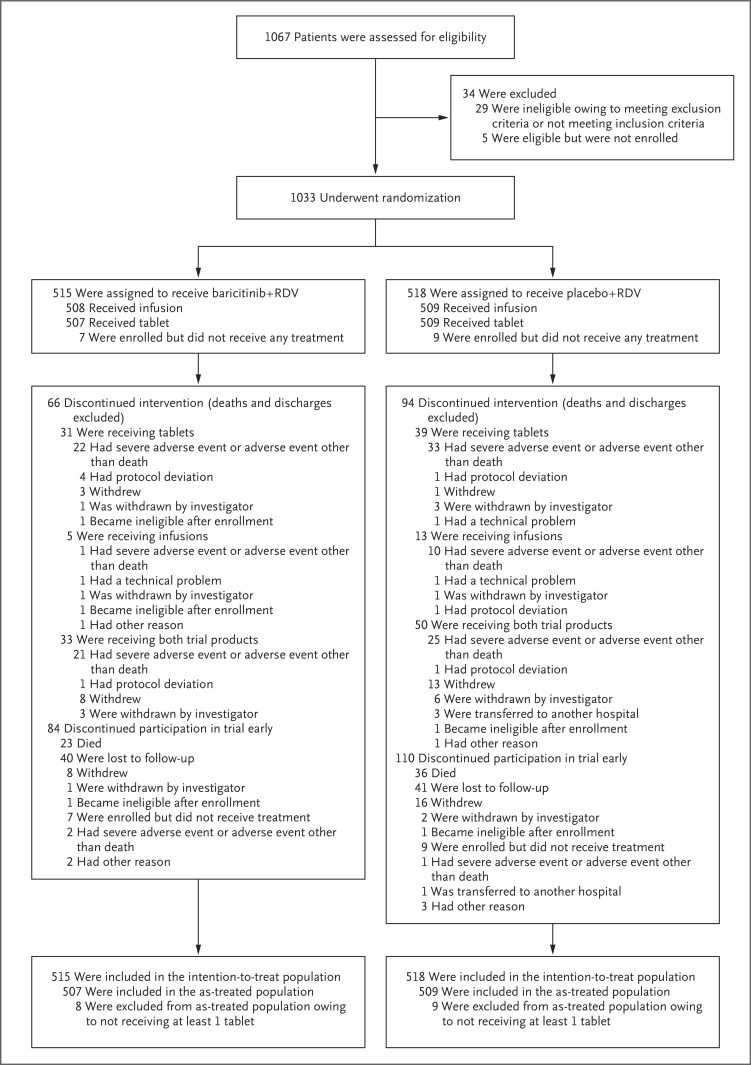
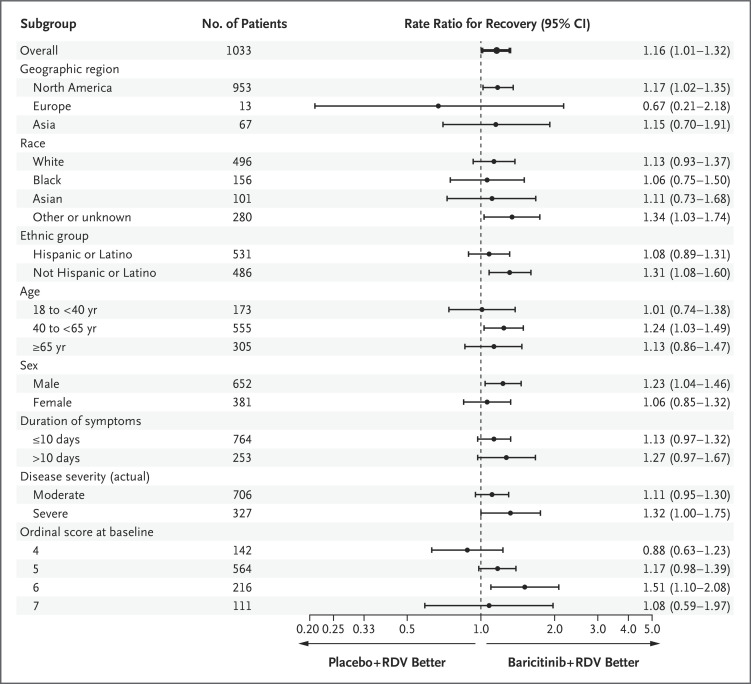
Results: A total of 1033 patients underwent randomization (with 515 assigned to combination treatment and 518 to control). Patients receiving baricitinib had a median time to recovery of 7 days (95% confidence interval [CI], 6 to 8), as compared with 8 days (95% CI, 7 to 9) with control (rate ratio for recovery, 1.16; 95% CI, 1.01 to 1.32; P = 0.03), and a 30% higher odds of improvement in clinical status at day 15 (odds ratio, 1.3; 95% CI, 1.0 to 1.6). Patients receiving high-flow oxygen or noninvasive ventilation at enrollment had a time to recovery of 10 days with combination treatment and 18 days with control (rate ratio for recovery, 1.51; 95% CI, 1.10 to 2.08). The 28-day mortality was 5.1% in the combination group and 7.8% in the control group (hazard ratio for death, 0.65; 95% CI, 0.39 to 1.09). Serious adverse events were less frequent in the combination group than in the control group (16.0% vs. 21.0%; difference, -5.0 percentage points; 95% CI, -9.8 to -0.3; P = 0.03), as were new infections (5.9% vs. 11.2%; difference, -5.3 percentage points; 95% CI, -8.7 to -1.9; P = 0.003).
Conclusions: Baricitinib plus remdesivir was superior to remdesivir alone in reducing recovery time and accelerating improvement in clinical status among patients with Covid-19, notably among those receiving high-flow oxygen or noninvasive ventilation. The combination was associated with fewer serious adverse events. (Funded by the National Institute of Allergy and Infectious Diseases; ClinicalTrials.gov number, NCT04401579.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Baricitinib Therapy in Covid-19 Pneumonia - An Unmet Need Fulfilled.N Engl J Med. 2021 Mar 4;384(9):867-869. doi: 10.1056/NEJMe2034982. N Engl J Med. 2021. PMID: 33657299 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- K08 AI143923/AI/NIAID NIH HHS/United States
- I01 BX003714/BX/BLRD VA/United States
- UM1 AI148685/AI/NIAID NIH HHS/United States
- UM1 AI148452/AI/NIAID NIH HHS/United States
- UM1 AI148573/AI/NIAID NIH HHS/United States
- UM1 AI148684/AI/NIAID NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- MC_UU_12023/22/MRC_/Medical Research Council/United Kingdom
- UL1 TR002645/TR/NCATS NIH HHS/United States
- R38 AI140299/AI/NIAID NIH HHS/United States
- UM1 AI148689/AI/NIAID NIH HHS/United States
- UM1 AI148450/AI/NIAID NIH HHS/United States
- UM1 AI148575/AI/NIAID NIH HHS/United States
- UM1 AI148576/AI/NIAID NIH HHS/United States
- UM1 TR004538/TR/NCATS NIH HHS/United States
- NCT04401579/US/United States/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases