

Vascular alterations among young adults with SARS-CoV-2
- PMID: 33306450
- PMCID: PMC8083172
- DOI: 10.1152/ajpheart.00897.2020
Vascular alterations among young adults with SARS-CoV-2
Abstract
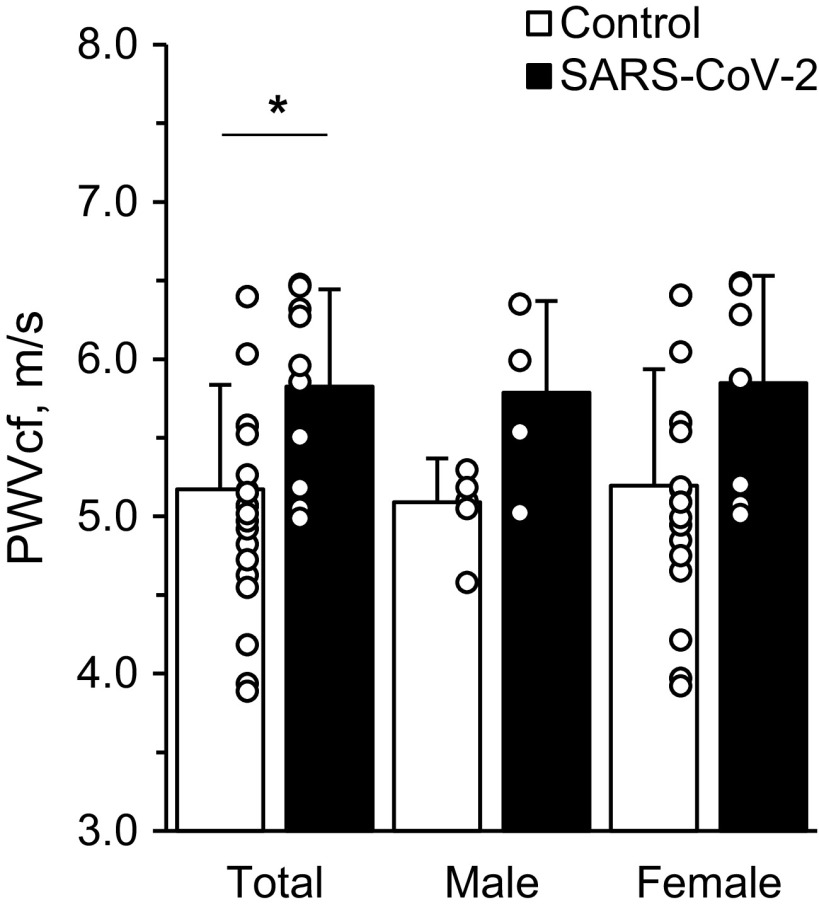
While SARS-CoV-2 primarily affects the lungs, the virus may be inflicting detriments to the cardiovascular system, both directly through angiotensin-converting enzyme 2 receptor and initiating systemic inflammation. Persistent systemic inflammation may be provoking vascular dysfunction, an early indication of cardiovascular disease risk. To establish the potential effects of SARS-CoV-2 on the systemic vasculature in the arms and legs, we performed a cross-sectional analysis of young healthy adults (control: 5 M/15 F, 23.0 ± 1.3 y, 167 ± 9 cm, 63.0 ± 7.4 kg) and young adults who, 3-4 wk prior to testing, had tested positive for SARS-CoV-2 (SARS-CoV-2: 4 M/7 F, 20.2 ± 1.1 y, 172 ± 12 cm, 69.5 ± 12.4 kg) (means ± SD). Using Doppler ultrasound, brachial artery flow-mediated dilation (FMD) in the arm and single passive limb movement (sPLM) in the leg were assessed as markers of vascular function. Carotid-femoral pulse wave velocity (PWVcf) was asvsessed as a marker of arterial stiffness. FMD was lower in the SARS-CoV-2 group (2.71 ± 1.21%) compared with the control group (8.81 ± 2.96%) (P < 0.01) and when made relative to the shear stimulus (SARS-CoV-2: 0.04 ± 0.02 AU, control: 0.13 ± 0.06 AU, P < 0.01). The femoral artery blood flow response, as evidenced by the area under the curve, from the sPLM was lower in the SARS-CoV-2 group (-3 ± 91 mL) compared with the control group (118 ± 114 mL) (P < 0.01). PWVcf was higher in the SARS-CoV-2 group (5.83 ± 0.62 m/s) compared with the control group (5.17 ± 0.66 m/s) (P < 0.01). Significantly lower systemic vascular function and higher arterial stiffness are evident weeks after testing positive for SARS-CoV-2 among young adults compared with controls.NEW & NOTEWORTHY This study was the first to investigate the vascular implications of contracting SARS-CoV-2 among young, otherwise healthy adults. Using a cross-sectional design, this study assessed vascular function 3-4 wk after young adults tested positive for SARS-CoV-2. The main findings from this study were a strikingly lower vascular function and a higher arterial stiffness compared with healthy controls. Together, these results suggest rampant vascular effects seen weeks after contracting SARS-CoV-2 in young adults.
Keywords: COVID-19; SARS-CoV-2; flow-mediated dilation; passive limb movement; pulse wave velocity.
Figures


Comment in
-
Vascular complications from SARS-CoV2: a unique finding or a common feature of viral infections?Am J Physiol Heart Circ Physiol. 2021 Jul 1;321(1):H253. doi: 10.1152/ajpheart.00249.2021. Am J Physiol Heart Circ Physiol. 2021. PMID: 34233135 Free PMC article. No abstract available.
References
-
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395: 1054–1062, 2020. doi: 10.1016/S0140-6736(20)30566-3. - DOI - PMC - PubMed
-
- Ferrario CM, Jessup J, Chappell MC, Averill DB, Brosnihan KB, Tallant EA, Diz DI, Gallagher PE. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation 111: 2605–2610, 2005. doi: 10.1161/CIRCULATIONAHA.104.510461. - DOI - PubMed
-
- Monteil V, Kwon H, Prado P, Hagelkruys A, Wimmer RA, Stahl M, Leopoldi A, Garreta E, Hurtado Del Pozo C, Prosper F, Romero JP, Wirnsberger G, Zhang H, Slutsky AS, Conder R, Montserrat N, Mirazimi A, Penninger JM. Inhibition of SARS-CoV-2 infections in engineered human tissues using clinical-grade soluble human ACE2. Cell 181: 905–913.e7, 2020. doi: 10.1016/j.cell.2020.04.004. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous