

Hospitalizations among adults with chronic kidney disease in the United States: A cohort study
- PMID: 33306688
- PMCID: PMC7732055
- DOI: 10.1371/journal.pmed.1003470
Hospitalizations among adults with chronic kidney disease in the United States: A cohort study
Abstract
Background: Adults with chronic kidney disease (CKD) are hospitalized more frequently than those without CKD, but the magnitude of this excess morbidity and the factors associated with hospitalizations are not well known.
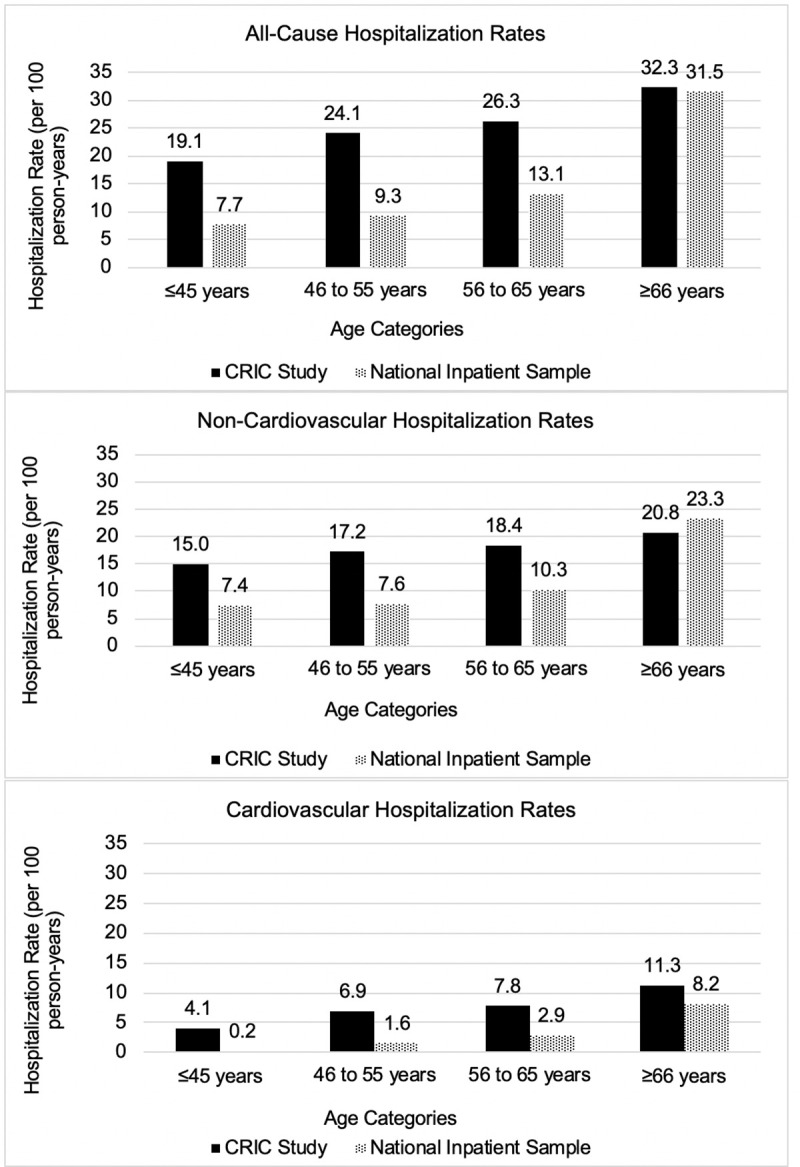
Methods and findings: Data from 3,939 participants enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study between 2003 and 2008 at 7 clinical centers in the United States were used to estimate primary causes of hospitalizations, hospitalization rates, and baseline participant factors associated with all-cause, cardiovascular, and non-cardiovascular hospitalizations during a median follow up of 9.6 years. Multivariable-adjusted Poisson regression was used to identify factors associated with hospitalization rates, including demographics, blood pressure, estimated glomerular filtration rate (eGFR), and proteinuria. Hospitalization rates in CRIC were compared with rates in the Nationwide Inpatient Sample (NIS) from 2012. Of the 3,939 CRIC participants, 45.1% were female, and 41.9% identified as non-Hispanic black, with a mean age of 57.7 years, and the mean eGFR is 44.9 ml/min/1.73m2. CRIC participants had an unadjusted overall hospitalization rate of 35.0 per 100 person-years (PY) [95% CI: 34.3 to 35.6] and 11.1 per 100 PY [95% CI: 10.8 to 11.5] for cardiovascular-related causes. All-cause, non-cardiovascular, and cardiovascular hospitalizations were associated with older age (≥65 versus 45 to 64 years), more proteinuria (≥150 to <500 versus <150 mg/g), higher systolic blood pressure (≥140 versus 120 to <130 mmHg), diabetes (versus no diabetes), and lower eGFR (<60 versus ≥60 ml/min/1.73m2). Non-Hispanic black (versus non-Hispanic white) race/ethnicity was associated with higher risk for cardiovascular hospitalization [rate ratio (RR) 1.25, 95% CI: 1.16 to 1.35, p-value < 0.001], while risk among females was lower [RR 0.89, 95% CI: 0.83 to 0.96, p-value = 0.002]. Rates of cardiovascular hospitalizations were higher among those with ≥500 mg/g of proteinuria irrespective of eGFR. The most common causes of hospitalization were related to cardiovascular (31.8%), genitourinary (8.7%), digestive (8.3%), endocrine, nutritional or metabolic (8.3%), and respiratory (6.7%) causes. Hospitalization rates were higher in CRIC than the NIS, except for non-cardiovascular hospitalizations among individuals aged >65 years. Limitations of the study include possible misclassification by diagnostic codes, residual confounding, and potential bias from healthy volunteer effect due to its observational nature.
Conclusions: In this study, we observed that adults with CKD had a higher hospitalization rate than the general population that is hospitalized, and even moderate reductions in kidney function were associated with elevated rates of hospitalization. Causes of hospitalization were predominantly related to cardiovascular disease, but other causes contributed, particularly, genitourinary, digestive, and endocrine, nutritional, and metabolic illnesses. High levels of proteinuria were observed to have the largest association with hospitalizations across a wide range of kidney function levels.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interest: EL receives consulting income from Acumen, LLC.
Figures




References
-
- System USRD. USRDS 2017 Annual Data Report: Atlas of Chornic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2017.
Publication types
MeSH terms
Grants and funding
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- K23 DK118198/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- R01 DK119199/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- K08 DK118213/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
