

Effects of a Household Air Pollution Intervention with Liquefied Petroleum Gas on Cardiopulmonary Outcomes in Peru. A Randomized Controlled Trial
- PMID: 33306939
- PMCID: PMC8456540
- DOI: 10.1164/rccm.202006-2319OC
Effects of a Household Air Pollution Intervention with Liquefied Petroleum Gas on Cardiopulmonary Outcomes in Peru. A Randomized Controlled Trial
Abstract
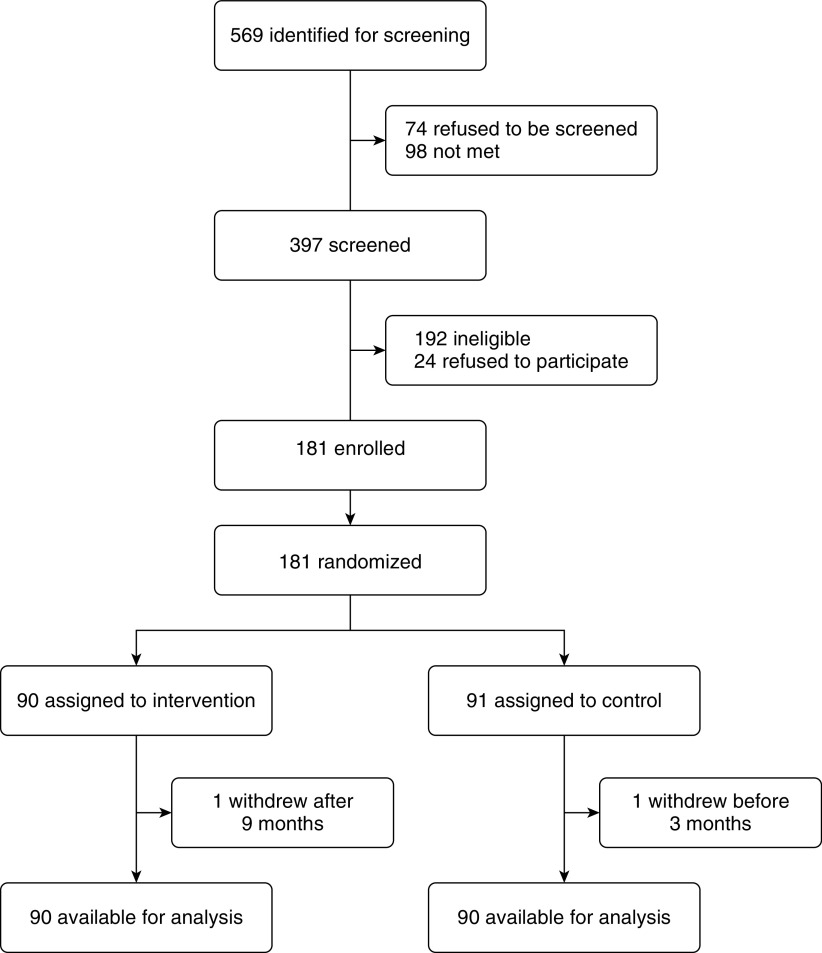
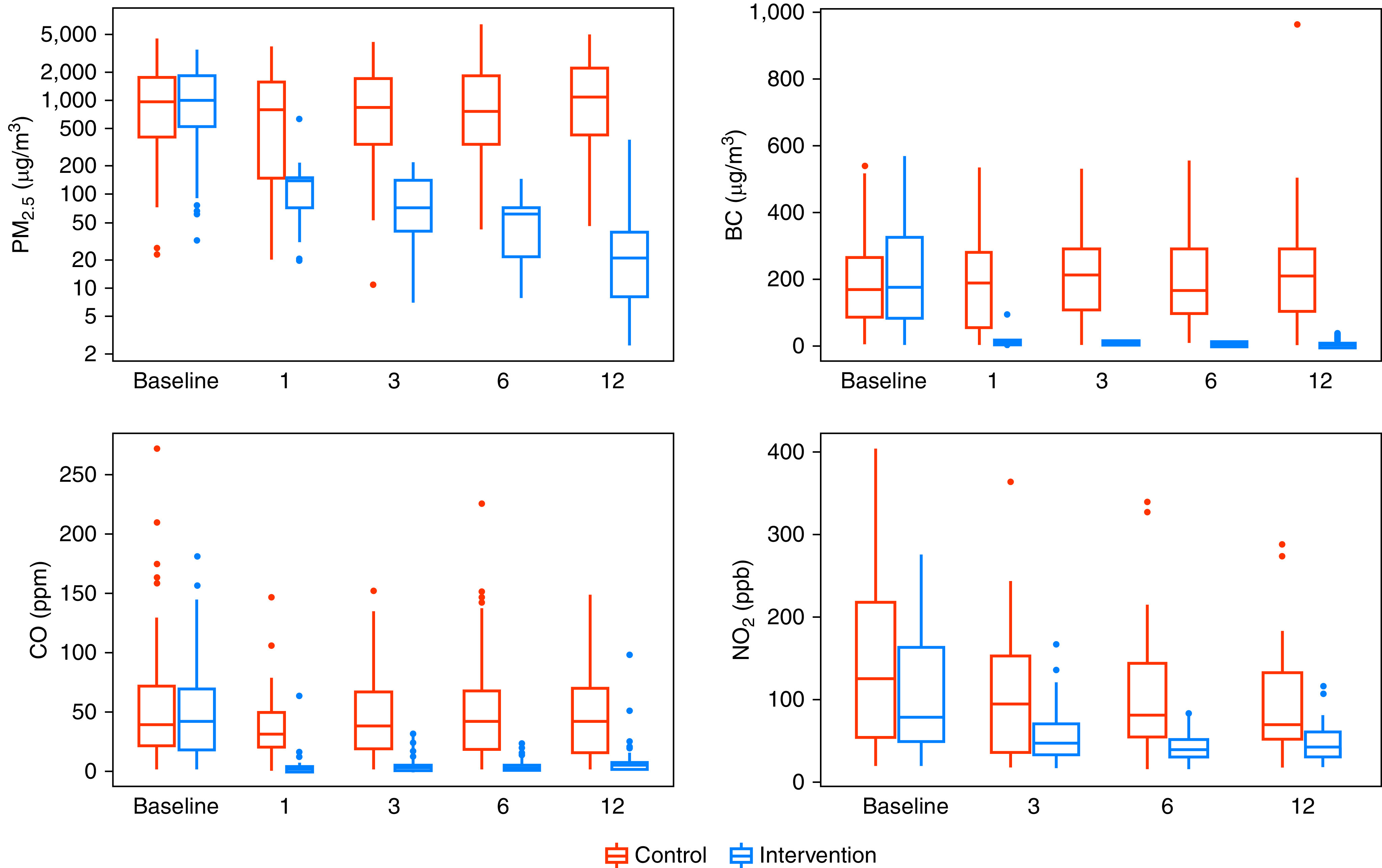
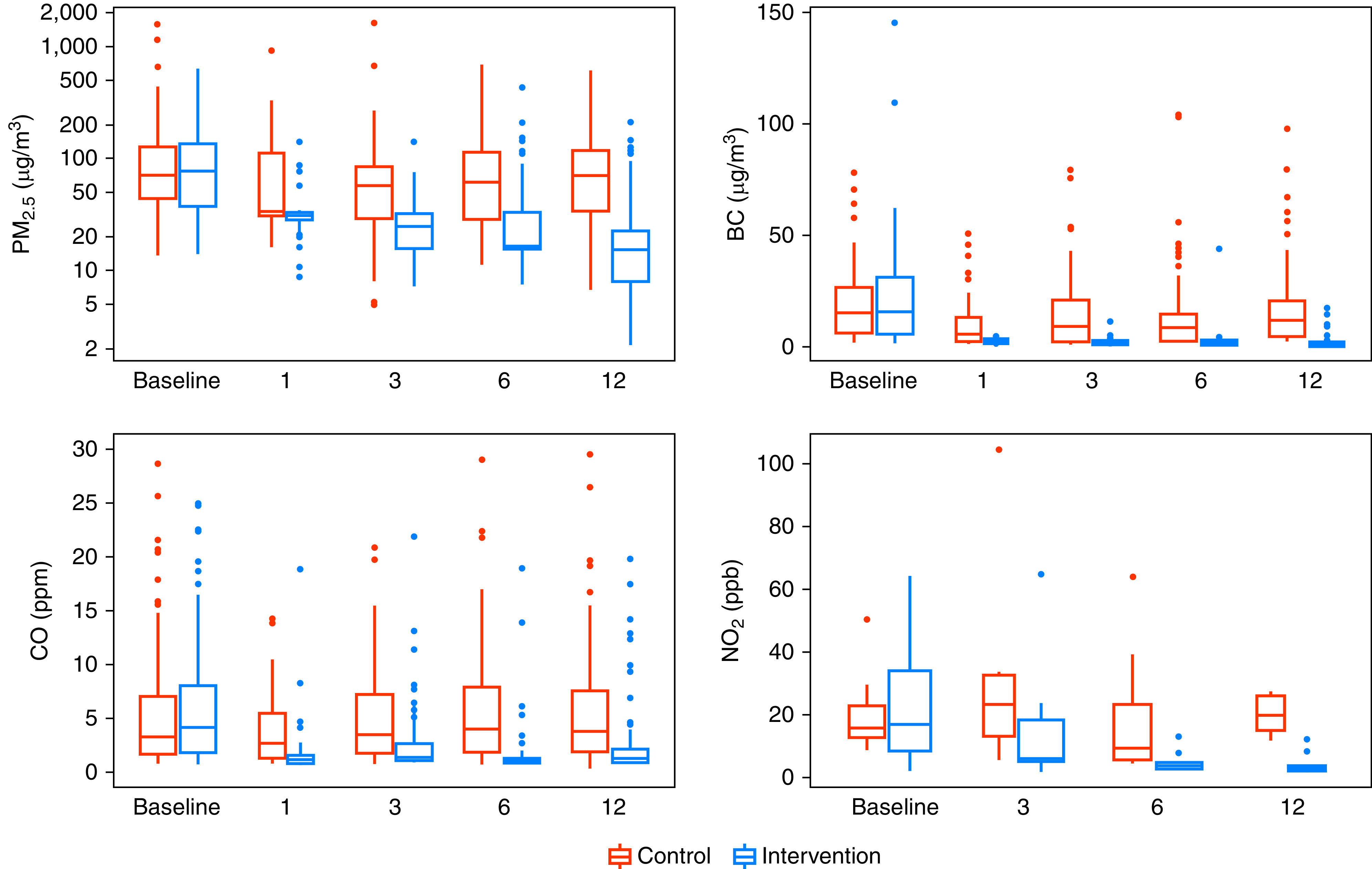
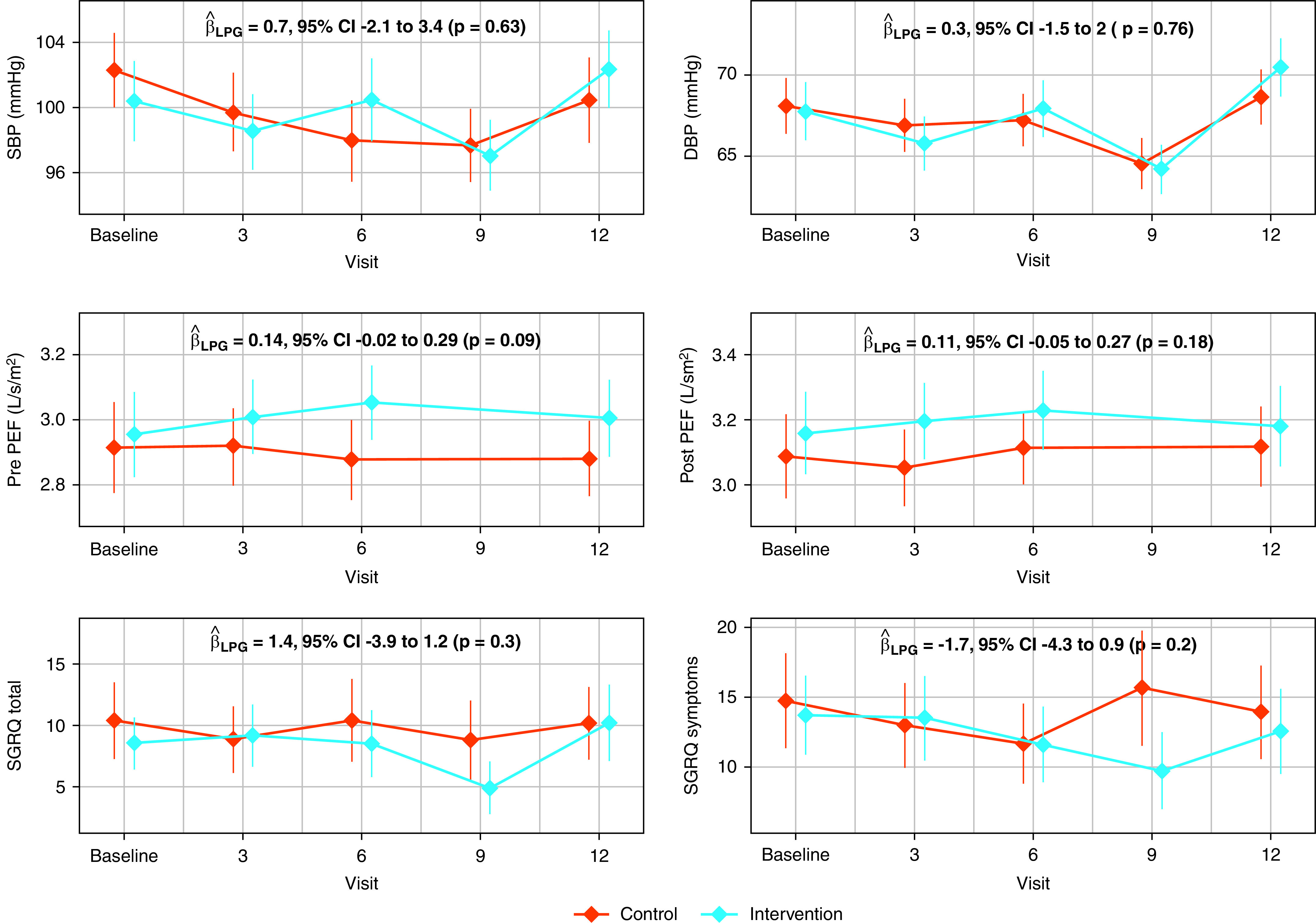
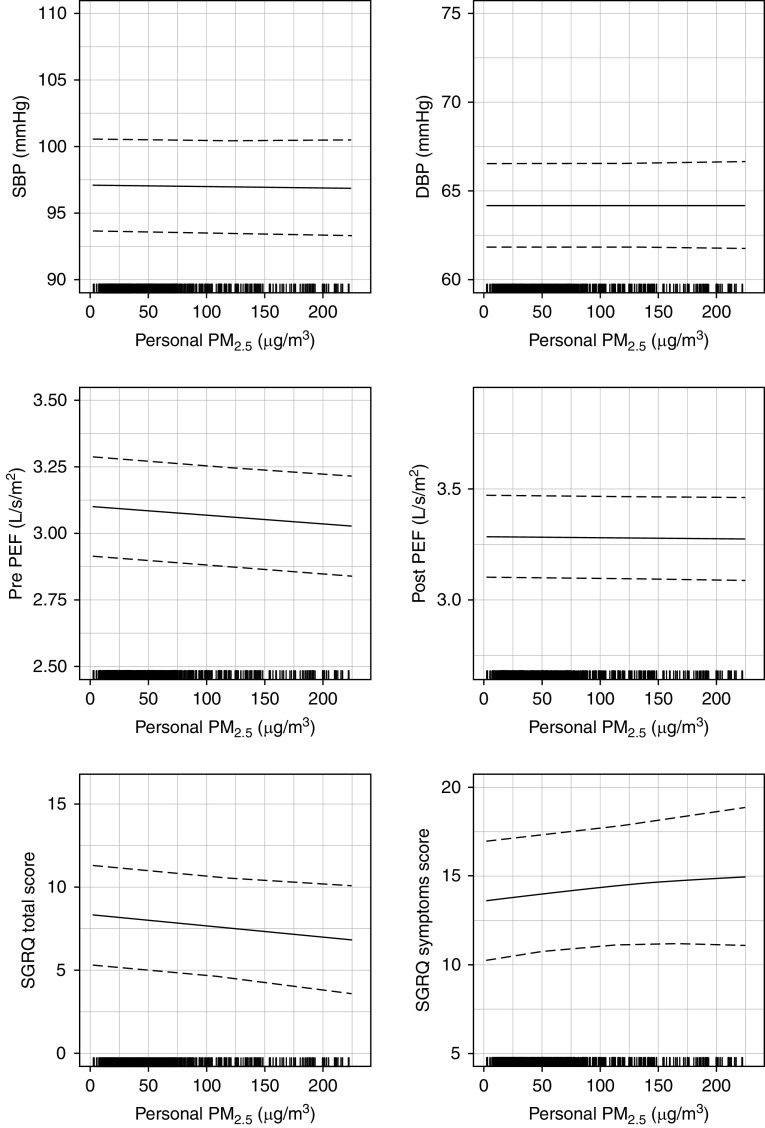
Rationale: Approximately 40% of people worldwide are exposed to household air pollution (HAP) from the burning of biomass fuels. Previous efforts to document health benefits of HAP mitigation have been stymied by an inability to lower emissions to target levels. Objectives: We sought to determine if a household air pollution intervention with liquefied petroleum gas (LPG) improved cardiopulmonary health outcomes in adult women living in a resource-poor setting in Peru. Methods: We conducted a randomized controlled field trial in 180 women aged 25-64 years living in rural Puno, Peru. Intervention women received an LPG stove, continuous fuel delivery for 1 year, education, and behavioral messaging, whereas control women were asked to continue their usual cooking practices. We assessed for stove use adherence using temperature loggers installed in both LPG and biomass stoves of intervention households. Measurements and Main Results: We measured blood pressure, peak expiratory flow (PEF), and respiratory symptoms using the St. George's Respiratory Questionnaire at baseline and at 3-4 visits after randomization. Intervention women used their LPG stove exclusively for 98% of days. We did not find differences in average postrandomization systolic blood pressure (intervention - control 0.7 mm Hg; 95% confidence interval, -2.1 to 3.4), diastolic blood pressure (0.3 mm Hg; -1.5 to 2.0), prebronchodilator peak expiratory flow/height2 (0.14 L/s/m2; -0.02 to 0.29), postbronchodilator peak expiratory flow/height2 (0.11 L/s/m2; -0.05 to 0.27), or St. George's Respiratory Questionnaire total score (-1.4; -3.9 to 1.2) over 1 year in intention-to-treat analysis. There were no reported harms related to the intervention. Conclusions: We did not find evidence of a difference in blood pressure, lung function, or respiratory symptoms during the year-long intervention with LPG. Clinical trial registered with www.clinicaltrials.gov (NCT02994680).
Keywords: blood pressure; household air pollution; lung function; respiratory symptoms.
Figures
Comment in
-
The Conundrum of Cleaner Cookstove Interventions: Necessary but Insufficient?Am J Respir Crit Care Med. 2021 Jun 1;203(11):1336-1338. doi: 10.1164/rccm.202012-4353ED. Am J Respir Crit Care Med. 2021. PMID: 33357118 Free PMC article. No abstract available.
References
-
- Zhang J, Smith KR. Indoor air pollution: a global health concern. Br Med Bull . 2003;68:209–225. - PubMed
-
- GBD 2017 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioral, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet . 2018;392:1923–1994. - PMC - PubMed
-
- Thakur M, Nuyts PAW, Boudewijns EA, Flores Kim J, Faber T, Babu GR, et al. Impact of improved cookstoves on women’s and child health in low and middle income countries: a systematic review and meta-analysis. Thorax . 2018;73:1026–1040. - PubMed
-
- Po JY, FitzGerald JM, Carlsten C. Respiratory disease associated with solid biomass fuel exposure in rural women and children: systematic review and meta-analysis. Thorax . 2011;66:232–239. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
