

The role of aspirin desensitization followed by oral aspirin therapy in managing patients with aspirin-exacerbated respiratory disease: A Work Group Report from the Rhinitis, Rhinosinusitis and Ocular Allergy Committee of the American Academy of Allergy, Asthma & Immunology
- PMID: 33307116
- PMCID: PMC7980229
- DOI: 10.1016/j.jaci.2020.10.043
The role of aspirin desensitization followed by oral aspirin therapy in managing patients with aspirin-exacerbated respiratory disease: A Work Group Report from the Rhinitis, Rhinosinusitis and Ocular Allergy Committee of the American Academy of Allergy, Asthma & Immunology
Abstract
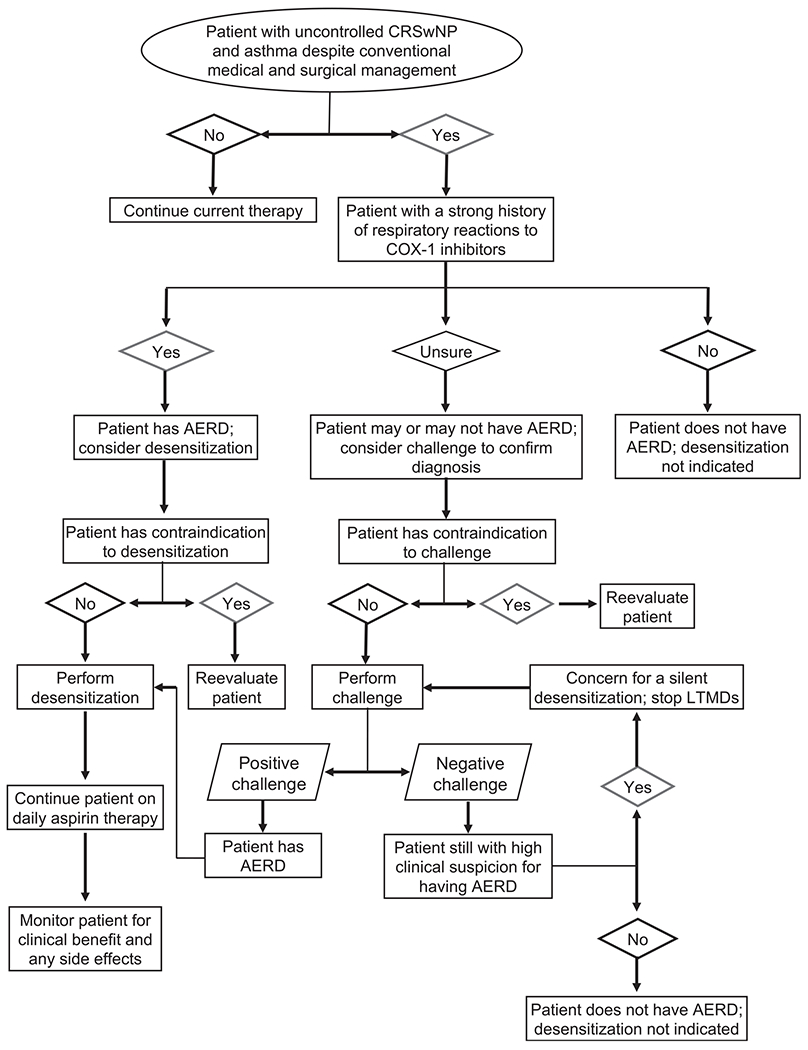
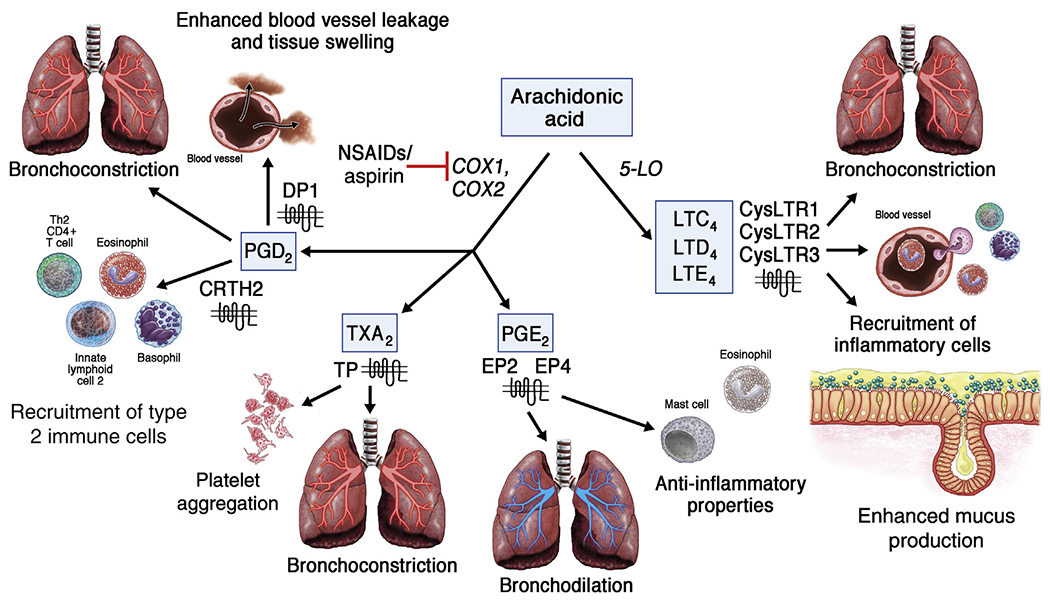
Aspirin-exacerbated respiratory disease (AERD) is characterized by the clinical triad of chronic rhinosinusitis with nasal polyps, asthma, and an intolerance to medications that inhibit the cycloxgenase-1 enzyme. Patients with AERD on average have more severe respiratory disease compared with patients with chronic rhinosinusitis with nasal polyps and/or asthma alone. Although patients with AERD traditionally develop significant upper and lower respiratory tract symptoms on ingestion of cycloxgenase-1 inhibitors, most of these same patients report clinical benefit when desensitized to aspirin and maintained on daily aspirin therapy. This Work Group Report provides a comprehensive review of aspirin challenges, aspirin desensitizations, and maintenance aspirin therapy in patients with AERD. Identification of appropriate candidates, indications and contraindications, medical and surgical optimization strategies, protocols, medical management during the desensitization, and recommendations for maintenance aspirin therapy following desensitization are reviewed. Also included is a summary of studies evaluating the clinical efficacy of aspirin therapy after desensitization as well as a discussion on the possible cellular and molecular mechanisms explaining how this therapy provides unique benefit to patients with AERD.
Keywords: AERD; Aspirin-exacerbated respiratory disease; NSAID-exacerbated respiratory disease; Samter triad; aspirin desensitization.
Copyright © 2020 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Roca-Ferrer J, Garcia-Garcia FJ, Pereda J, Perez-Gonzalez M, Pujols L, Alobid I, et al. Reduced expression of COXs and production of prostaglandin E(2) in patients with nasal polyps with or without aspirin-intolerant asthma. J Allergy Clin Immunol 2011;128:66–72.e1. - PubMed
-
- Christie PE, Tagari P, Ford-Hutchinson AW, Charlesson S, Chee P, Arm JP, et al. Urinary leukotriene E4 concentrations increase after aspirin challenge in aspirin-sensitive asthmatic subjects. Am Rev Respir Dis 1991;143:1025–9. - PubMed
-
- Perez-Novo CA, Watelet JB, Claeys C, Van Cauwenberge P, Bachert C. Prostaglandin, leukotriene, and lipoxin balance in chronic rhinosinusitis with and without nasal polyposis. J Allergy Clin Immunol 2005;115:1189–96. - PubMed
-
- Rajan JP, Wineinger NE, Stevenson DD, White AA. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: a meta-analysis of the literature. J Allergy Clin Immunol 2015;135:676–81.e1. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
