

Reference ranges ("normal values") for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update
- PMID: 33308262
- PMCID: PMC7734766
- DOI: 10.1186/s12968-020-00683-3
Reference ranges ("normal values") for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update
Erratum in
-
Correction to: Reference ranges ("normal values") for cardiovascular magnetic resonance (CMR) in adults and children: 2020 update.J Cardiovasc Magn Reson. 2021 Oct 18;23(1):114. doi: 10.1186/s12968-021-00815-3. J Cardiovasc Magn Reson. 2021. PMID: 34663334 Free PMC article. No abstract available.
Abstract
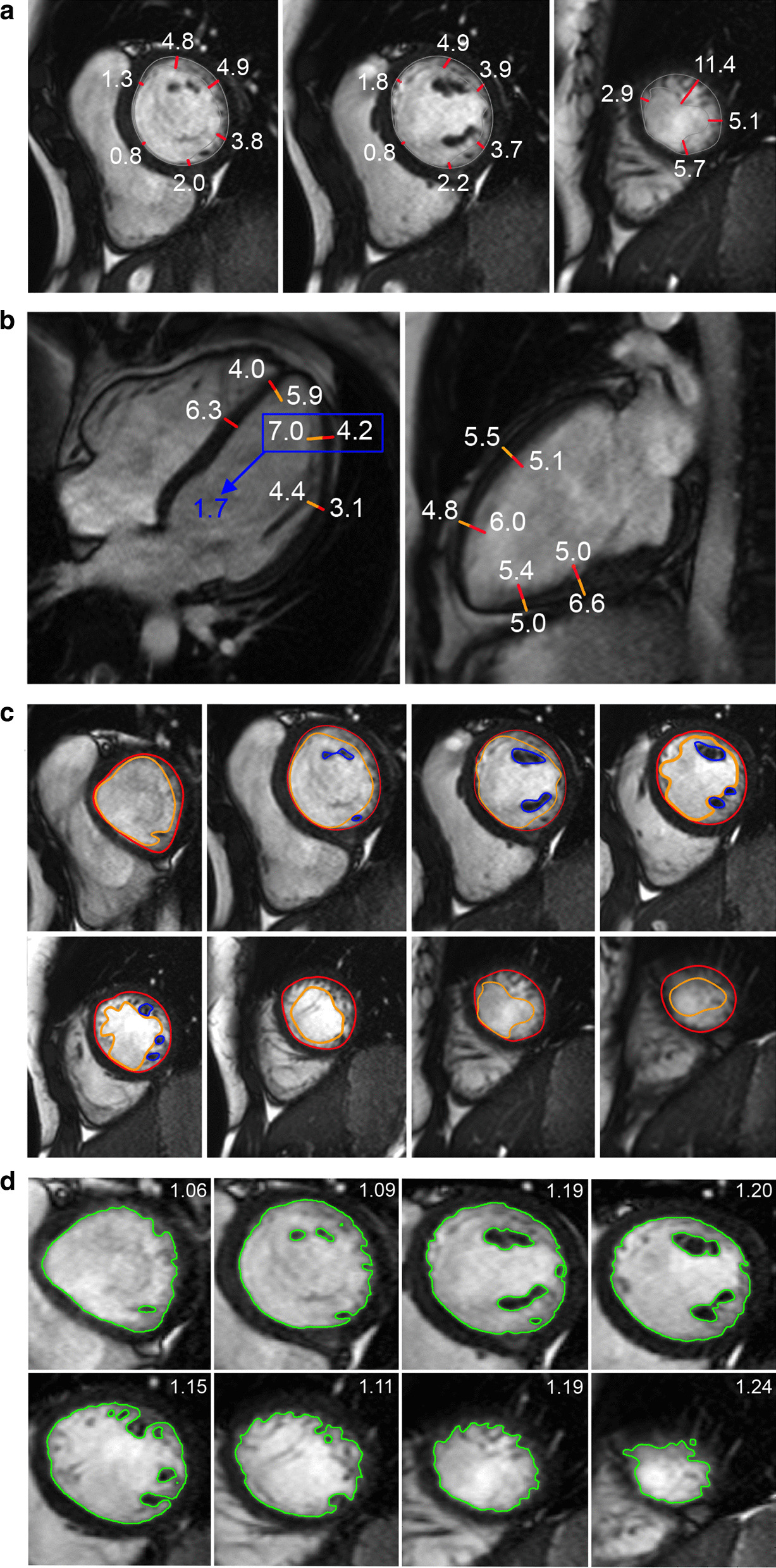
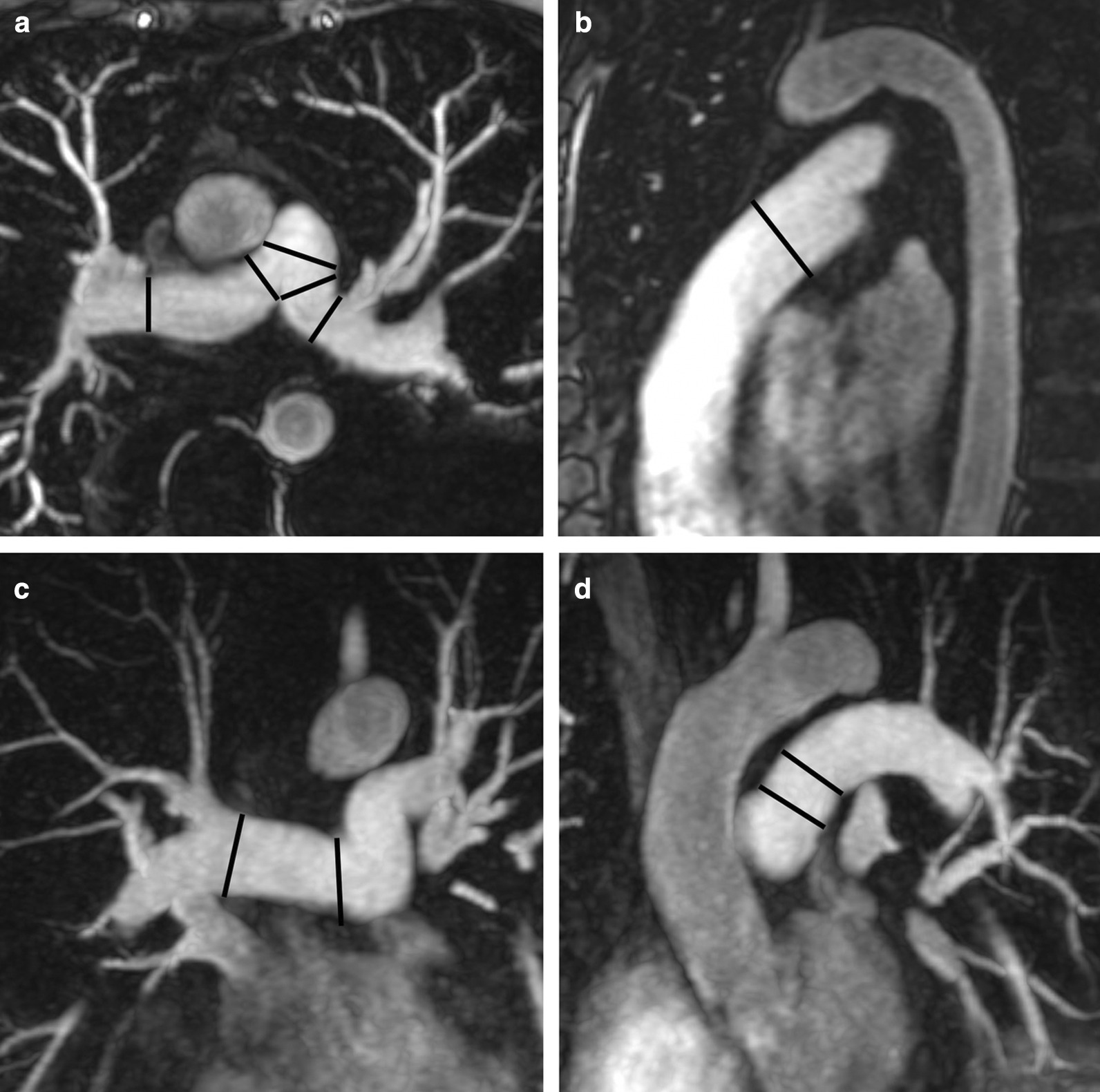
Cardiovascular magnetic resonance (CMR) enables assessment and quantification of morphological and functional parameters of the heart, including chamber size and function, diameters of the aorta and pulmonary arteries, flow and myocardial relaxation times. Knowledge of reference ranges ("normal values") for quantitative CMR is crucial to interpretation of results and to distinguish normal from disease. Compared to the previous version of this review published in 2015, we present updated and expanded reference values for morphological and functional CMR parameters of the cardiovascular system based on the peer-reviewed literature and current CMR techniques. Further, databases and references for deep learning methods are included.
Keywords: Cardiac magnetic resonance; Normal values; Reference range.
Conflict of interest statement
CJF: Research support by GE healthcare. MS: Research support by Siemens healthcare. SDT: Boehringer Ingelheim speaker bureau.
Figures











References
-
- Tao Q, Yan W, Wang Y, Paiman EHM, Shamonin DP, Garg P, Plein S, Huang L, Xia L, Sramko M, et al. Deep Learning-based Method for Fully Automatic Quantification of Left Ventricle Function from Cine MR Images: A Multivendor Multicenter Study. Radiology. 2019;290:81–88. doi: 10.1148/radiol.2018180513. - DOI - PubMed
-
- SCMR: Consensus/Position statements, [https://scmr.org/general/custom.asp?page=guidelines], Accessed 15 Dec 2019
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
