

Radical surgery versus organ preservation via short-course radiotherapy followed by transanal endoscopic microsurgery for early-stage rectal cancer (TREC): a randomised, open-label feasibility study
- PMID: 33308452
- PMCID: PMC7802515
- DOI: 10.1016/S2468-1253(20)30333-2
Radical surgery versus organ preservation via short-course radiotherapy followed by transanal endoscopic microsurgery for early-stage rectal cancer (TREC): a randomised, open-label feasibility study
Abstract
Background: Radical surgery via total mesorectal excision might not be the optimal first-line treatment for early-stage rectal cancer. An organ-preserving strategy with selective total mesorectal excision could reduce the adverse effects of treatment without substantially compromising oncological outcomes. We investigated the feasibility of recruiting patients to a randomised trial comparing an organ-preserving strategy with total mesorectal excision.
Methods: TREC was a randomised, open-label feasibility study done at 21 tertiary referral centres in the UK. Eligible participants were aged 18 years or older with rectal adenocarcinoma, staged T2 or lower, with a maximum diameter of 30 mm or less; patients with lymph node involvement or metastases were excluded. Patients were randomly allocated (1:1) by use of a computer-based randomisation service to undergo organ preservation with short-course radiotherapy followed by transanal endoscopic microsurgery after 8-10 weeks, or total mesorectal excision. Where the transanal endoscopic microsurgery specimen showed histopathological features associated with an increased risk of local recurrence, patients were considered for planned early conversion to total mesorectal excision. A non-randomised prospective registry captured patients for whom randomisation was considered inappropriate, because of a strong clinical indication for one treatment group. The primary endpoint was cumulative randomisation at 12, 18, and 24 months. Secondary outcomes evaluated safety, efficacy, and health-related quality of life assessed with the European Organisation for Research and Treatment of Cancer (EORTC) QLQ C30 and CR29 in the intention-to-treat population. This trial is registered with the ISRCTN Registry, ISRCTN14422743.
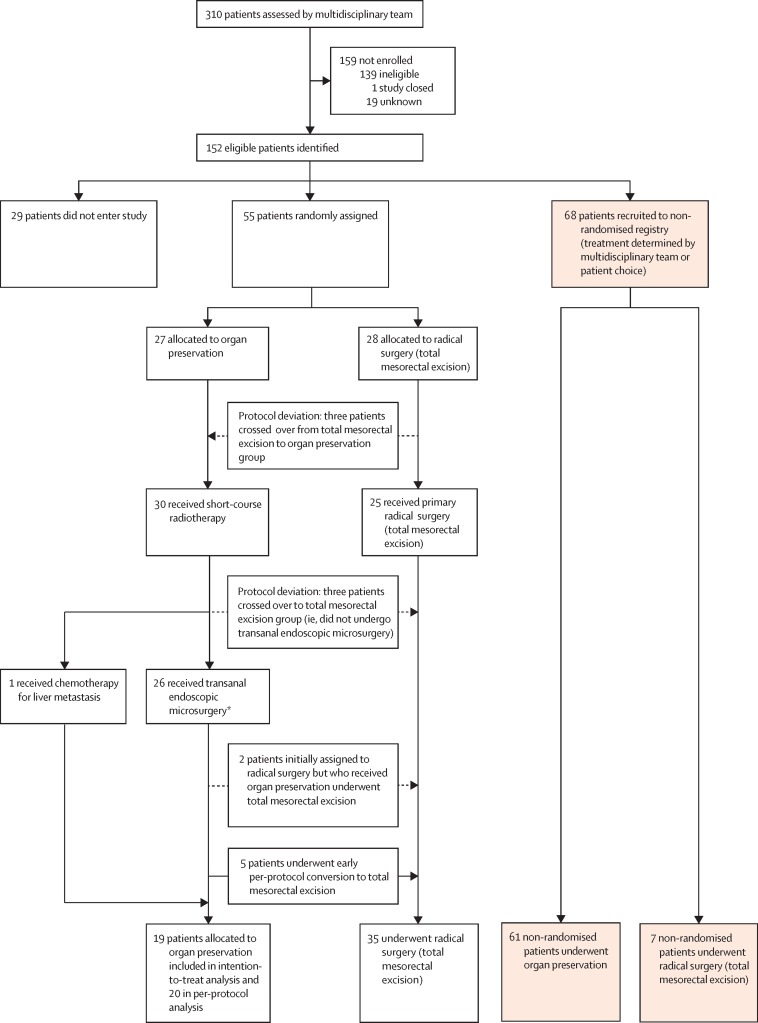
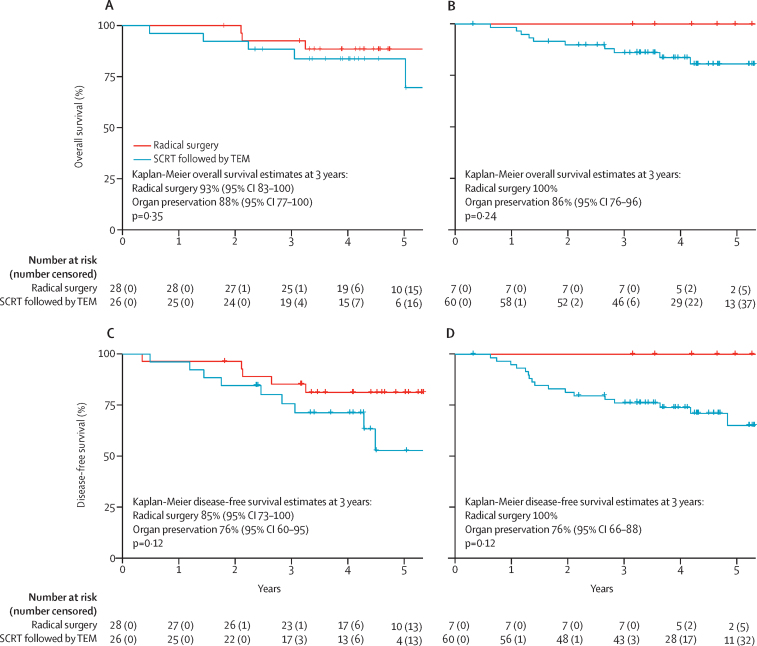
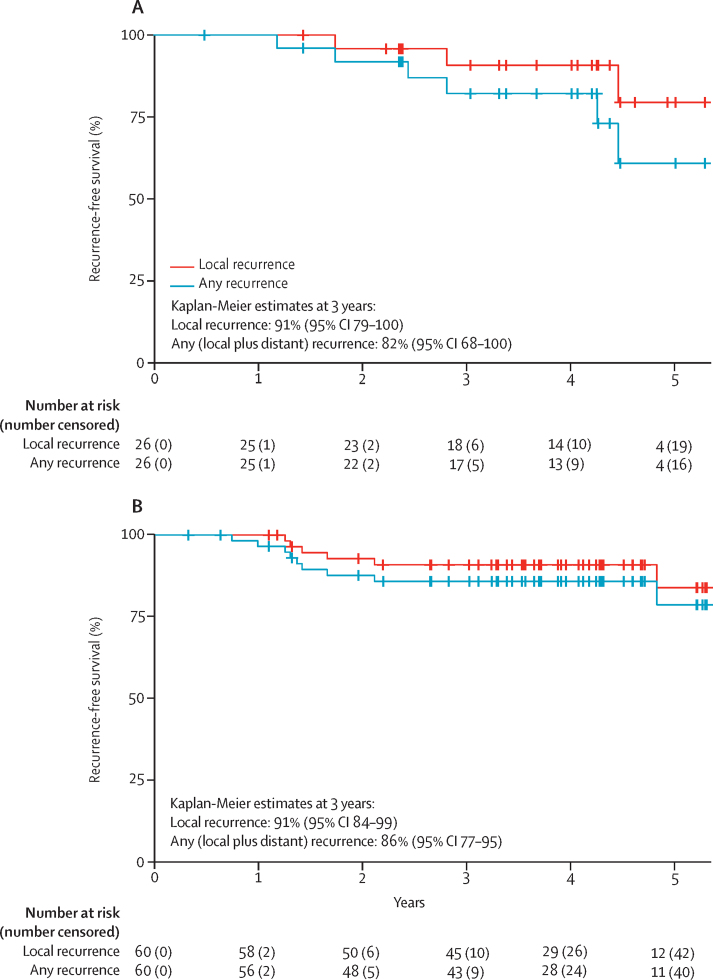
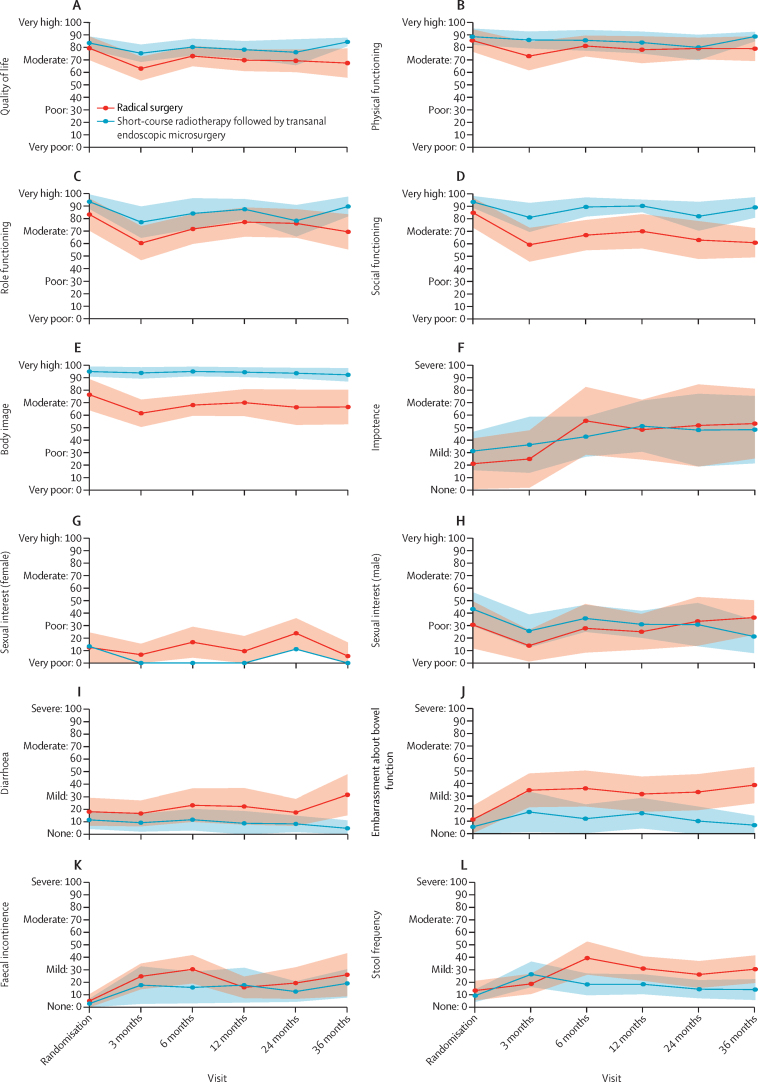
Findings: Between Feb 22, 2012, and Dec 19, 2014, 55 patients were randomly assigned at 15 sites; 27 to organ preservation and 28 to radical surgery. Cumulatively, 18 patients had been randomly assigned at 12 months, 31 at 18 months, and 39 at 24 months. No patients died within 30 days of initial treatment, but one patient randomly assigned to organ preservation died within 6 months following conversion to total mesorectal excision with anastomotic leakage. Eight (30%) of 27 patients randomly assigned to organ preservation were converted to total mesorectal excision. Serious adverse events were reported in four (15%) of 27 patients randomly assigned to organ preservation versus 11 (39%) of 28 randomly assigned to total mesorectal excision (p=0·04, χ2 test). Serious adverse events associated with organ preservation were most commonly due to rectal bleeding or pain following transanal endoscopic microsurgery (reported in three cases). Radical total mesorectal excision was associated with medical and surgical complications including anastomotic leakage (two patients), kidney injury (two patients), cardiac arrest (one patient), and pneumonia (two patients). Histopathological features that would be considered to be associated with increased risk of tumour recurrence if observed after transanal endoscopic microsurgery alone were present in 16 (59%) of 27 patients randomly assigned to organ preservation, versus 24 (86%) of 28 randomly assigned to total mesorectal excision (p=0·03, χ2 test). Eight (30%) of 27 patients assigned to organ preservation achieved a complete response to radiotherapy. Patients who were randomly assigned to organ preservation showed improvements in patient-reported bowel toxicities and quality of life and function scores in multiple items compared to those who were randomly assigned to total mesorectal excision, which were sustained over 36 months' follow-up. The non-randomised registry comprised 61 patients who underwent organ preservation and seven who underwent radical surgery. Non-randomised patients who underwent organ preservation were older than randomised patients and more likely to have life-limiting comorbidities. Serious adverse events occurred in ten (16%) of 61 non-randomised patients who underwent organ preservation versus one (14%) of seven who underwent total mesorectal excision. 24 (39%) of 61 non-randomised patients who underwent organ preservation had high-risk histopathological features, while 25 (41%) of 61 achieved a complete response. Overall, organ preservation was achieved in 19 (70%) of 27 randomised patients and 56 (92%) of 61 non-randomised patients.
Interpretation: Short-course radiotherapy followed by transanal endoscopic microsurgery achieves high levels of organ preservation, with relatively low morbidity and indications of improved quality of life. These data support the use of organ preservation for patients considered unsuitable for primary total mesorectal excision due to the short-term risks associated with this surgery, and support further evaluation of short-course radiotherapy to achieve organ preservation in patients considered fit for total mesorectal excision. Larger randomised studies, such as the ongoing STAR-TREC study, are needed to more precisely determine oncological outcomes following different organ preservation treatment schedules.
Funding: Cancer Research UK.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Moving forward with organ preservation in rectal cancer.Lancet Gastroenterol Hepatol. 2021 Feb;6(2):82-83. doi: 10.1016/S2468-1253(20)30390-3. Epub 2020 Dec 11. Lancet Gastroenterol Hepatol. 2021. PMID: 33308451 No abstract available.
-
Radical surgery versus organ preservation for early-stage rectal cancer.Lancet Gastroenterol Hepatol. 2021 Apr;6(4):263. doi: 10.1016/S2468-1253(21)00015-7. Lancet Gastroenterol Hepatol. 2021. PMID: 33714365 No abstract available.
-
Radical surgery versus organ preservation for early-stage rectal cancer - Authors' reply.Lancet Gastroenterol Hepatol. 2021 Apr;6(4):263-264. doi: 10.1016/S2468-1253(21)00061-3. Lancet Gastroenterol Hepatol. 2021. PMID: 33714366 No abstract available.
-
[Organ preservation after short-course radiotherapy and transanal endoscopic microsurgery for early-stage rectal cancer (TREC)].Strahlenther Onkol. 2021 Aug;197(8):749-751. doi: 10.1007/s00066-021-01795-0. Epub 2021 Jun 4. Strahlenther Onkol. 2021. PMID: 34089100 Free PMC article. German. No abstract available.
References
-
- Gollins S, Moran B, Adams R. Association of Coloproctology of Great Britain & Ireland (ACPGBI): guidelines for the management of cancer of the colon, rectum and anus (2017) —multidisciplinary management. Colorectal Dis. 2017;19(suppl 1):37–66. - PubMed
-
- Boyle J, Braun M, Hill J. National Bowel Cancer Audit: annual report 2018. December, 2018. https://www.nboca.org.uk/reports/annual-report-2018/
-
- Gilbert A, Ziegler L, Martland M. Systematic review of radiation therapy toxicity reporting in randomized controlled trials of rectal cancer: a comparison of patient-reported outcomes and clinician toxicity reporting. Int J Radiat Oncol Biol Phys. 2015;92:555–567. - PubMed
-
- Wiltink LM, Marijnen CA, Meershoek-Klein Kranenbarg E, van de Velde CJ, Nout RA. A comprehensive longitudinal overview of health-related quality of life and symptoms after treatment for rectal cancer in the TME trial. Acta Oncol. 2016;55:502–508. - PubMed
-
- Dossa F, Acuna SA, Baxter NN. Local excision after preoperative chemoradiation for T2 and T3 rectal cancers: is the wait over? Lancet Gastroenterol Hepatol. 2020;5:422–424. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
