

Review
doi: 10.1016/S0140-6736(20)31559-2.
Retinal vascular occlusions
Affiliations
- PMID: 33308475
- PMCID: PMC9546635
- DOI: 10.1016/S0140-6736(20)31559-2
Item in Clipboard
Review
Retinal vascular occlusions
Lancet.
.
Abstract
Acute retinal vascular occlusions are common causes of visual impairment. Although both retinal artery occlusions and retinal vein occlusions are associated with increased age and cardiovascular risk factors, their pathophysiology, systemic implications, and management differ substantially. Acute management of retinal artery occlusions involves a multidisciplinary approach including neurologists with stroke expertise, whereas treatment of retinal vein occlusions is provided by ophthalmologists. Optimisation of systemic risk factors by patients' primary care providers is an important component of the management of these two disorders.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
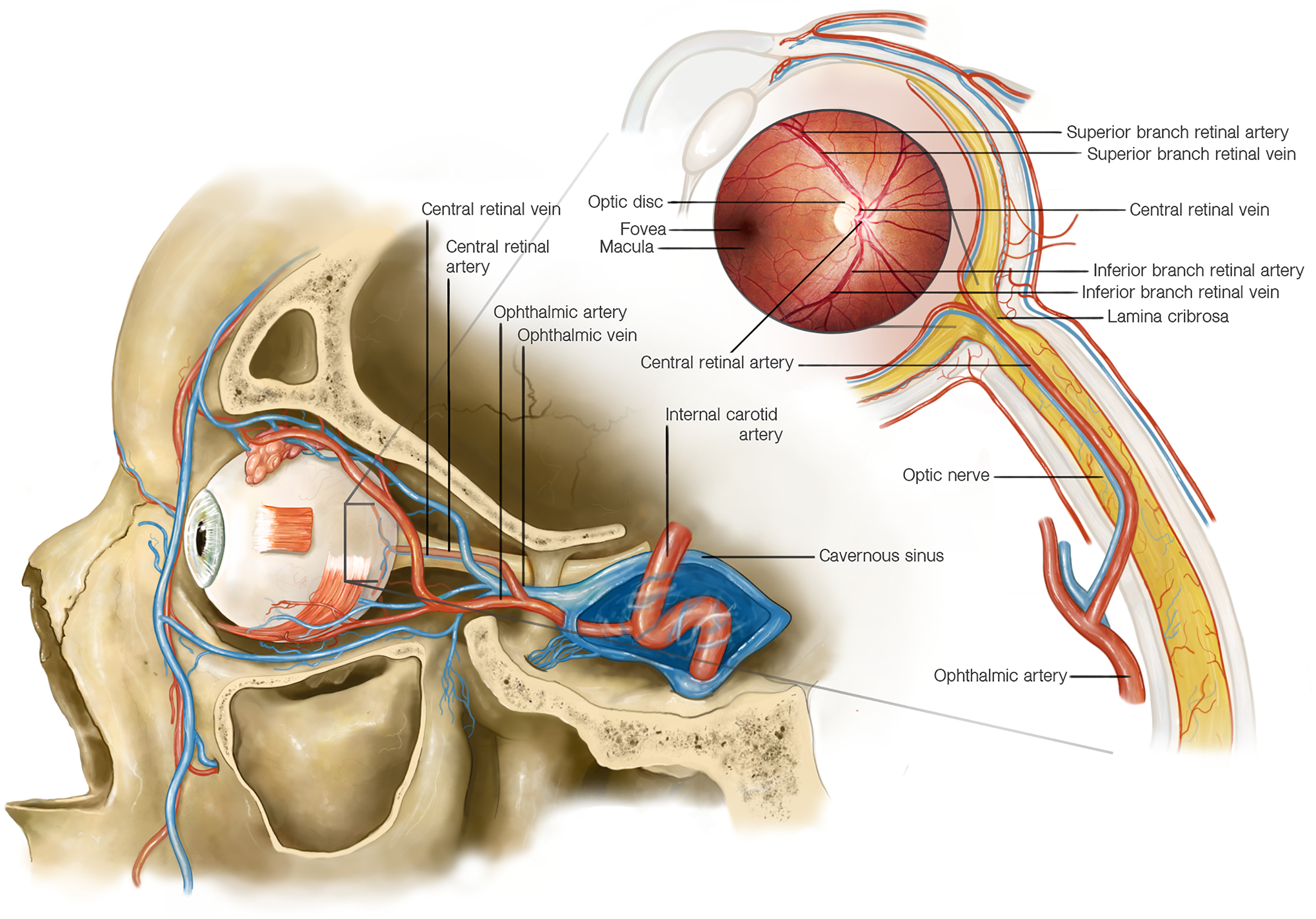
The arterial blood supply to the eye comes mostly from vascular networks originating from the ophthalmic artery, the most distal branch of the internal carotid artery. The central retinal artery is a branch of the ophthalmic artery that enters the optic nerve approximately 10–12 mm behind the eye and supplies the inner layers of the retina. At the level of the optic nerve head the central retinal artery divides into superior and inferior branches. The outer layers of the retina are supplied by the choroidal arteries, which originate from the posterior ciliary arteries (also branches of the ophthalmic artery). The retinal veins follow the retinal arteries, and the superior and inferior retinal veins join at the level of the optic disc where the central retinal vein enters the optic nerve, adjacent to the central retinal artery. The central retinal vein travels posteriorly in the optic nerve and exits the optic nerve in close proximity to the central retinal artery to join the superior and inferior ophthalmic veins which drain into the cavernous sinus. Both the central retinal artery and vein travel though the lamina cribrosa, a mesh-like connective tissue structure at the level of the scleral canal. The optic nerve is vascularized by a different circulation derived from the ophthalmic artery: the posterior part of the optic nerve is supplied by a surrounding pial plexus originating from small branches off the ophthalmic artery posteriorly and from the posterior ciliary arteries anteriorly; the optic nerve head receives its arterial blood supply from an anastomotic arterial circle (the circle of Zinn–Haller), formed by anastomoses among side branches of the short posterior ciliary arteries, branches from the nearby pial arterial network, and branches from choroidal vessels.
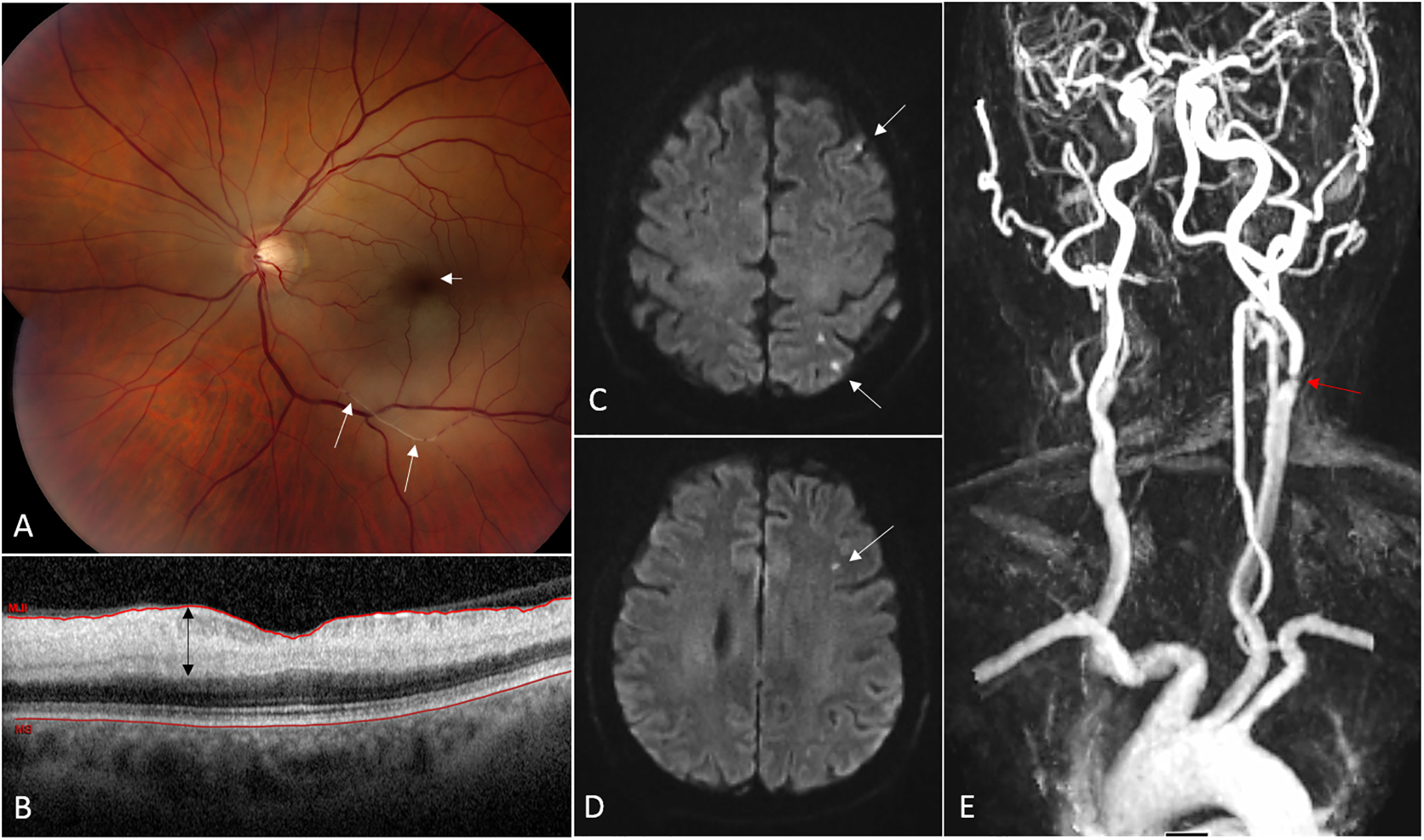
(A) Fundus photograph from a 68 year-old man with acute CRAO in the left eye. The ischemic retina appears whitish and the normally perfused fovea (from the choroidal circulation) is dark red in contrast, consistent with a so-called “cherry-red spot” (short arrow). Platelet-fibrin emboli are seen migrating in the inferior branches of the central retinal artery (long arrows). (B) Optical coherence tomography (OCT) of the macula showing a cut through the fovea. The ischemic inner retinal layers are thickened (black arrow) whereas the outer retinal layers are normal. (C, D) Brain MRI (axial cuts, diffusion-weighted images) performed 24 hours after onset of visual loss demonstrates multiple small acute areas of infarction as small hypersignals in the left hemisphere (arrows). (E) Magnetic resonance imaging (MRA) of the neck and great vessels shows a severe atheromatous stenosis at the origin of the left internal carotid artery.
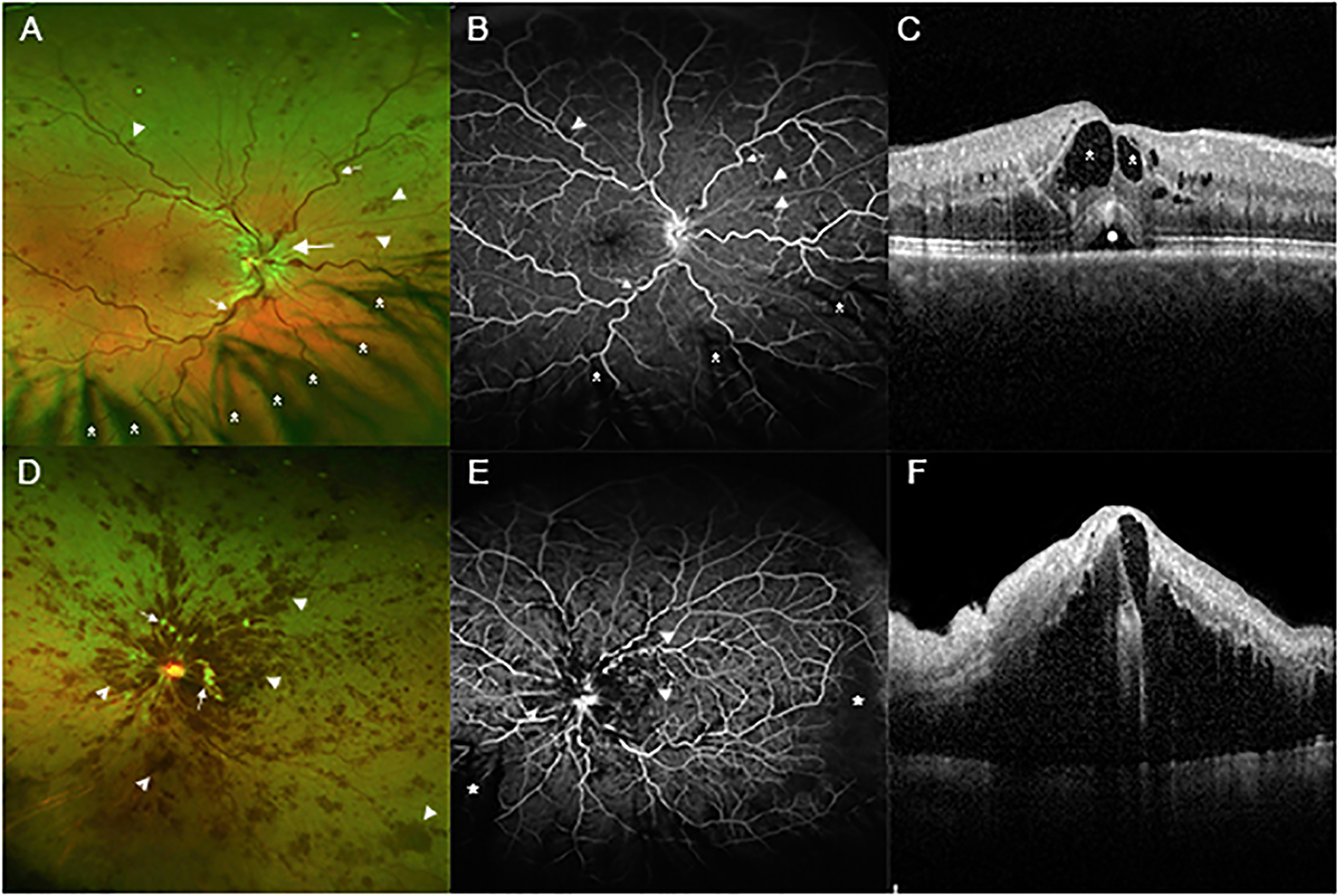
(A) A wide angle fundus photograph from a patient who presented with a mild CRVO shows dilated and tortuous retinal veins (small arrows), edema of the optic disc and surrounding retina (large arrow), and small hemorrhages scattered in all 4 quadrants of the retina (arrowheads). There is eye lash artifact inferiorly due to shadows cast on the retina from the eye lashes (asterisks). (B) Fluorescein angiography of same patient shows tortuous veins (small arrows) and blocked fluorescence from the small hemorrhages (arrowheads). The retinal capillaries are well-perfused throughout the posterior retina. Most of the dark areas inferiorly are due to shadowing from eye lashes (asterisks). (C) A spectral domain optical coherence tomography (SD-OCT) scan through the fovea shows intraretinal fluid (dark spaces within the retina, asterisks) and a small collection of fluid under the retina (circle). (D) A wide angle fundus photograph from a patient who presented with a moderately severe CRVO shows retinal hemorrhages (arrowheads) which are confluent in the posterior pole and scattered throughout the peripheral retina. There are several white cotton wool patches caused by infarcts in the nerve fiber layer (small arrows). (E) Fluorescein angiography shows blocked fluorescence from the retinal hemorrhages (arrowheads) and retinal nonperfusion (RNP) temporally and inferonasally (asterisks). (F) SD-OCT through the fovea shows massive edema.
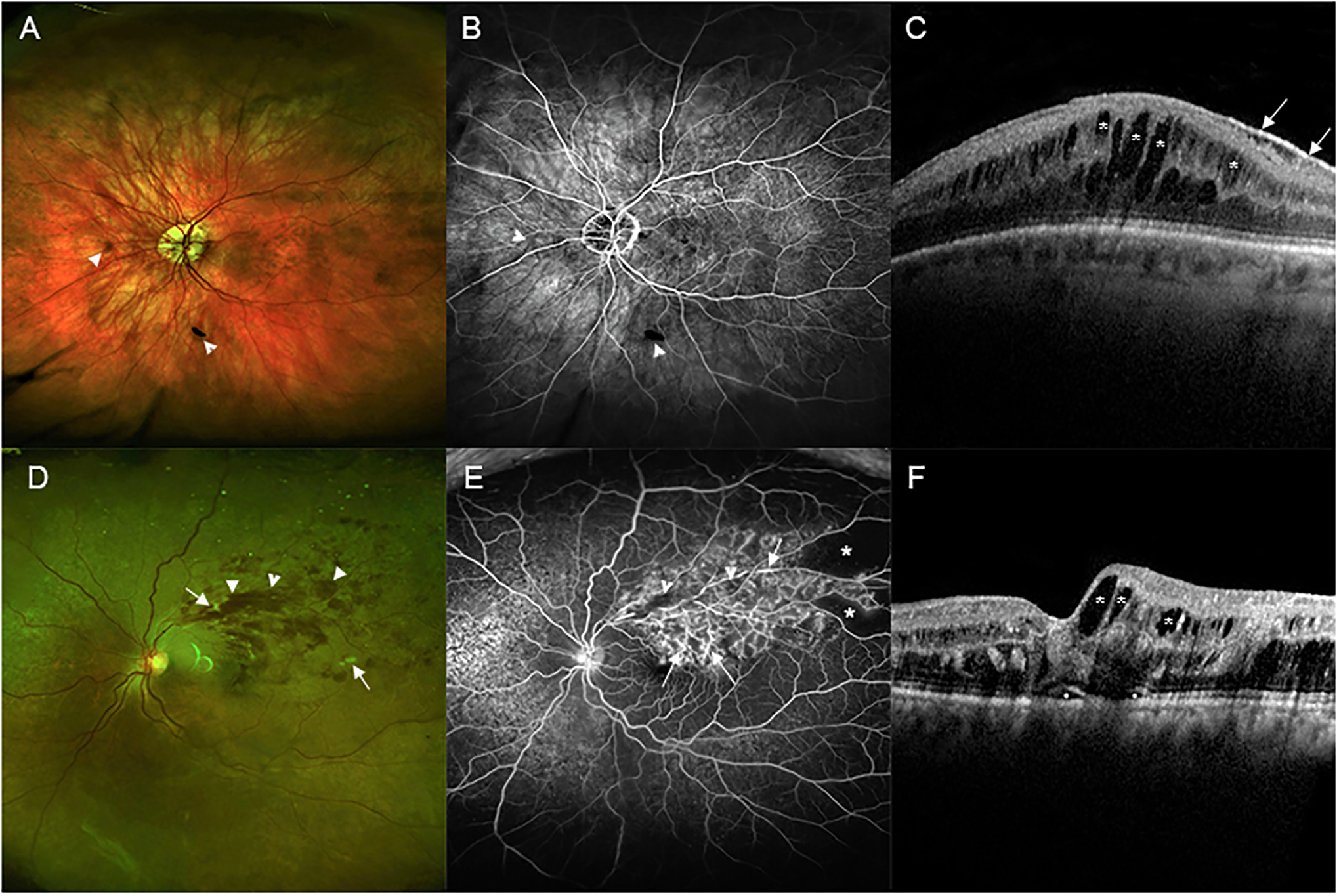
(A) A wide angle fundus photograph from a patient who presented with a mild BRVO shows only a few small hemorrhages (arrowheads). (B) Fluorescein angiography shows blocked fluorescence from hemorrhages (arrowheads) and good retinal perfusion. The dark area superiorly is sometimes seen at the edge of an image due to inadequate pupillary dilation and is not RNP. (C) A spectral domain optical coherence tomography (SD-OCT) scan through the fovea shows many dark cystoid spaces (asterisks). The white line along the surface is an epiretinal membrane that is incidental to the BRVO and is not visually significant (small arrows). (D) A wide angle fundus photograph from a patient who presented with a moderately severe BRVO shows retinal hemorrhages extending from the site of occlusion out to the periphery of the superotemporal retina (arrowheads). There are a few cotton wool patches (small arrows). (E) Fluorescein angiography shows mild blocked fluorescence from retinal hemorrhages (arrowheads) and staining of vessel walls (arrows) throughout the region drained by the occluded vein with RNP in the periphery (asterisks). (F) SD-OCT shows small areas (circles) of fluid under the fovea and cystoid spaces of intraretinal fluid (asterisks) that are larger temporal to the fovea than nasal to the fovea.
References
-
- Central Vein Occlusion Study Group. Natural history and clinical management of central retinal vein occlusion. The Central Vein Occlusion Study Group. Arch Ophthalmol 1997; 115: 486–91. - PubMed
-
- Ponto KA, Scharrer I, Binder H, et al. Hypertension and multiple cardiovascular risk factors increase the risk for retinal vein occlusions: results from the Gutenberg Retina lVein Occlusion Study J Hypertension 2019; 37: 1372–83. - PubMed
-
- Biousse V, Nahab F, Newman NJ. Management of acute retinal ischemia. Follow the guidelines! Ophthalmology 2018; 125: 1597–607. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
