

A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER)
- PMID: 33309278
- PMCID: PMC10262981
- DOI: 10.1016/j.eururo.2020.11.010
A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER)
Abstract
Context: Management of locally recurrent prostate cancer after definitive radiotherapy remains controversial due to the perceived high rates of severe genitourinary (GU) and gastrointestinal (GI) toxicity associated with any local salvage modality.
Objective: To quantitatively compare the efficacy and toxicity of salvage radical prostatectomy (RP), high-intensity focused ultrasound (HIFU), cryotherapy, stereotactic body radiotherapy (SBRT), low-dose-rate (LDR) brachytherapy, and high-dose-rate (HDR) brachytherapy.
Evidence acquisition: We performed a systematic review of PubMed, EMBASE, and MEDLINE. Two- and 5-yr recurrence-free survival (RFS) rates and crude incidences of severe GU and GI toxicity were extracted as endpoints of interest. Random-effect meta-analyses were conducted to characterize summary effect sizes and quantify heterogeneity. Estimates for each modality were then compared with RP after adjusting for individual study-level covariates using mixed-effect regression models, while allowing for differences in between-study variance across treatment modalities.
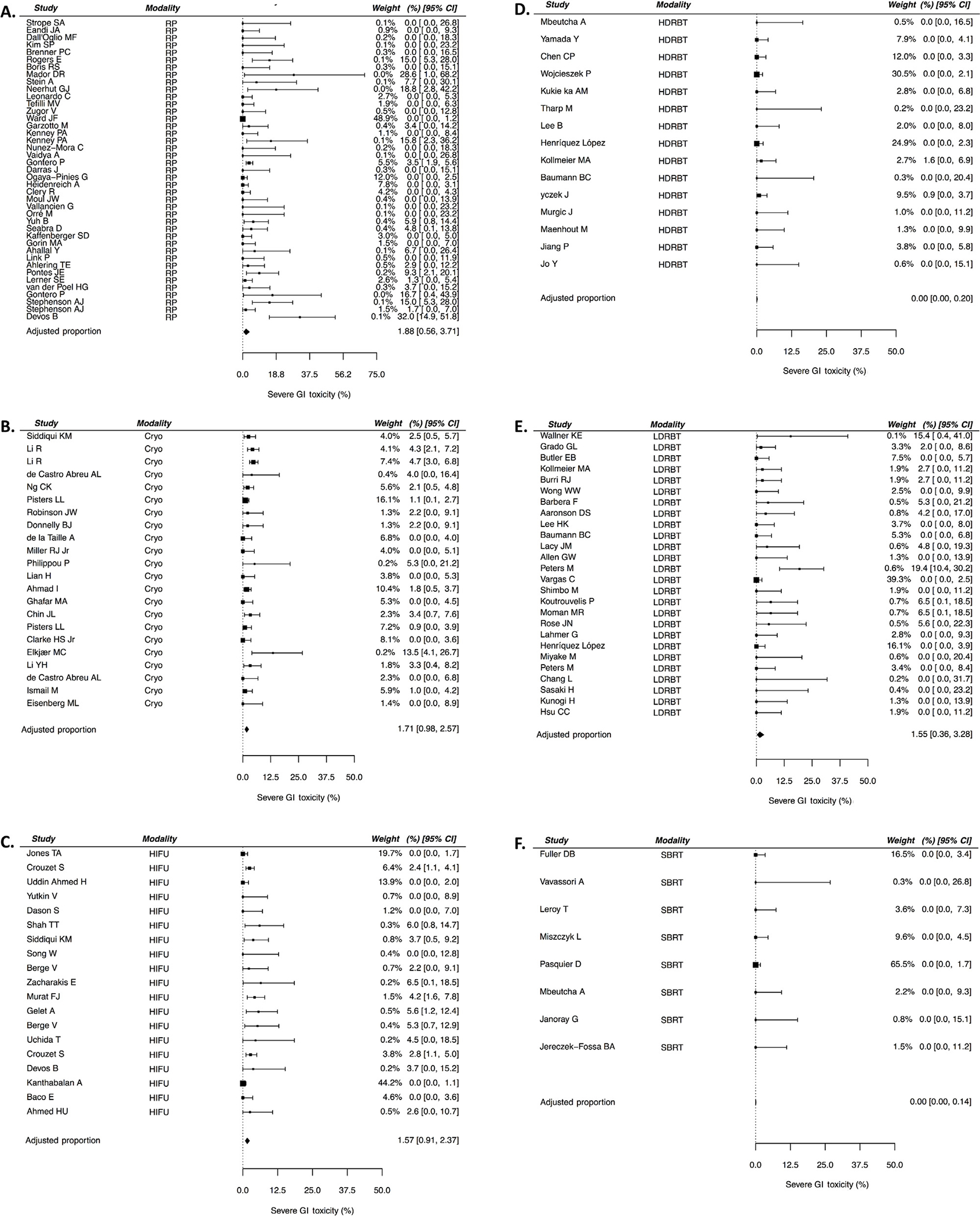
Evidence synthesis: A total of 150 studies were included for analysis. There was significant heterogeneity between studies within each modality, and covariates differed between modalities, necessitating adjustment. Adjusted 5-yr RFS ranged from 50% after cryotherapy to 60% after HDR brachytherapy and SBRT, with no significant differences between any modality and RP. Severe GU toxicity was significantly lower with all three forms of radiotherapeutic salvage than with RP (adjusted rates of 20% after RP vs 5.6%, 9.6%, and 9.1% after SBRT, HDR brachytherapy, and LDR brachytherapy, respectively; p ≤ 0.001 for all). Severe GI toxicity was significantly lower with HDR salvage than with RP (adjusted rates 1.8% vs 0.0%, p < 0.01), with no other differences identified.
Conclusions: Large differences in 5-yr outcomes were not uncovered when comparing all salvage treatment modalities against RP. Reirradiation with SBRT, HDR brachytherapy, or LDR brachytherapy appears to result in less severe GU toxicity than RP, and reirradiation with HDR brachytherapy yields less severe GI toxicity than RP. Prospective studies of local salvage for radiorecurrent disease are warranted.
Patient summary: In a large study-level meta-analysis, we looked at treatment outcomes and toxicity for men treated with a number of salvage treatments for radiorecurrent prostate cancer. We conclude that relapse-free survival at 5 years is equivalent among salvage modalities, but reirradiation may lead to lower toxicity.
Keywords: Cryotherapy; High-dose-rate brachytherapy; High-intensity focused ultrasound; Low–dose-rate brachytherapy; Meta-analysis; Prostate cancer; Radiation therapy; Radical prostatectomy; Radiorecurrent prostate cancer; Salvage therapy; Stereotactic body radiotherapy.
Copyright © 2020 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures



Comment in
-
Reply to Sungeun Kim, Jae Il Shin, and Jonathan Evan Shoag's Letter to the Editor re: Luca F. Valle, Eric J. Lehrer, Daniela Markovic, et al. A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur Urol. In press. https://doi.org/10.1016/j.eururo.2020.11.010.Eur Urol. 2021 Jul;80(1):e15-e16. doi: 10.1016/j.eururo.2021.04.010. Epub 2021 Apr 29. Eur Urol. 2021. PMID: 33934928 No abstract available.
-
Re: Luca F. Valle, Eric J. Lehrer, Daniela Markovic, et al. A Systematic Review and Meta-analysis of Local Salvage Therapies After Radiotherapy for Prostate Cancer (MASTER). Eur Urol. In press. https://doi.org/10.1016/j.eururo.2020.11.010.Eur Urol. 2021 Jul;80(1):e14. doi: 10.1016/j.eururo.2021.04.011. Epub 2021 Apr 30. Eur Urol. 2021. PMID: 33941402 No abstract available.
-
Mastering the Landscape of Postradiation Local Prostate Salvage Therapy.Eur Urol. 2021 Sep;80(3):293-294. doi: 10.1016/j.eururo.2021.04.032. Epub 2021 May 15. Eur Urol. 2021. PMID: 34006445 No abstract available.
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: prostate cancer. Version I.2019; ed2019. - PubMed
-
- Roach M 3rd, Hanks G, Thames H Jr, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 2006;65:965–74. - PubMed
