

Prevalence of Comorbid Asthma and Related Outcomes in COVID-19: A Systematic Review and Meta-Analysis
- PMID: 33309934
- PMCID: PMC7725230
- DOI: 10.1016/j.jaip.2020.11.054
Prevalence of Comorbid Asthma and Related Outcomes in COVID-19: A Systematic Review and Meta-Analysis
Abstract
Background: The impact of asthma on coronavirus disease 2019 (COVID-19) remains largely unknown.
Objective: To investigate the asthma prevalence among patients with COVID-19 and compare outcomes between patients with and without asthma.
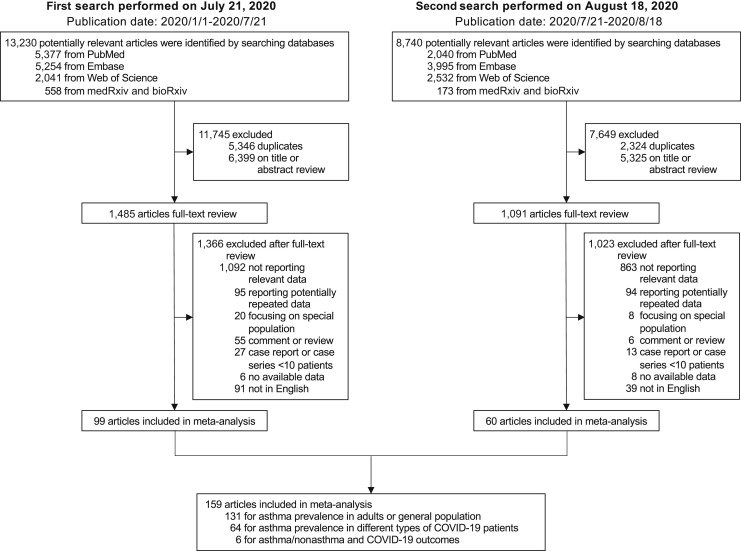
Methods: In this systematic review and meta-analysis, we searched PubMed, Embase, Web of Science, bioRxiv, and medRxiv for studies reporting asthma prevalence in general patients with COVID-19 or comparing outcomes between patients with and without asthma, and excluded duplicate publications, reviews, editorials, comments, single case reports, or small case series (<10 cases). We determined the pooled estimates of effect using random-effect model.
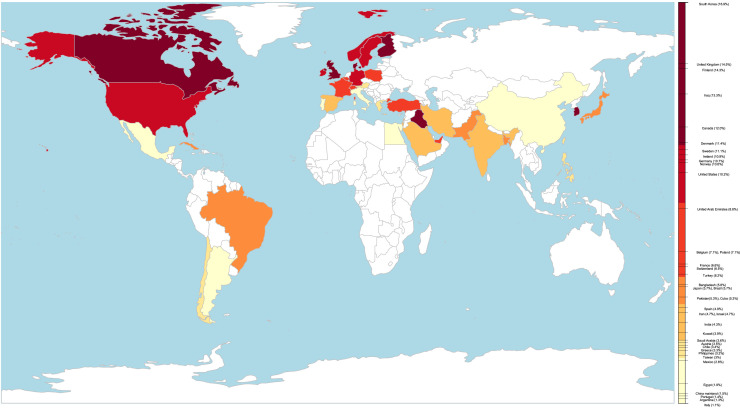
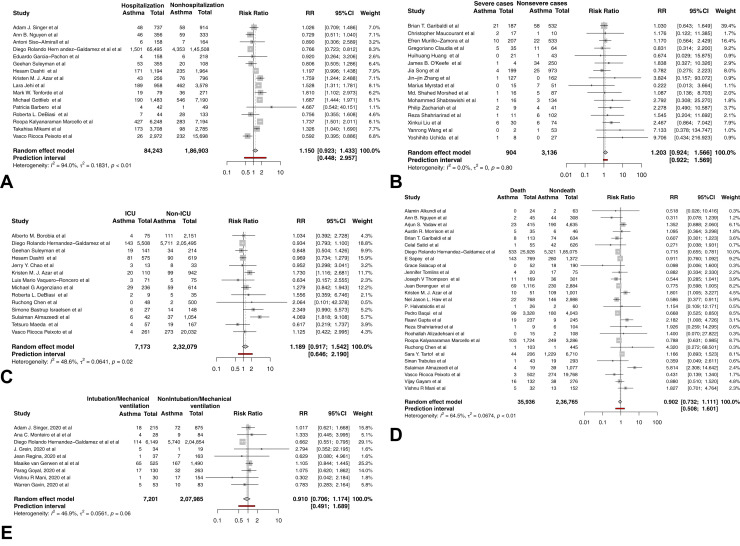
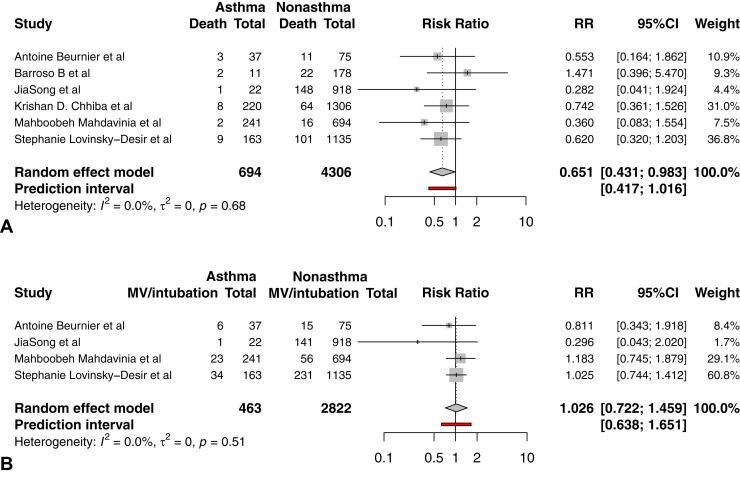
Results: On the basis of 131 studies (410,382 patients), we found great variability in the prevalence of comorbid asthma among patients with COVID-19 in different countries or regions ranging from 1.1% to 16.9%. No significant difference in asthma prevalence was found between hospitalized and nonhospitalized (risk ratio [RR], 1.15; 95% CI, 0.92-1.43), severe and nonsevere (RR, 1.21; 95% CI, 0.92-1.57), intensive care unit and non-intensive care unit (RR, 1.19; 95% CI, 0.92-1.54), dead and survived (RR, 0.90; 95% CI, 0.73-1.11), intubated/mechanically ventilated and nonintubated/mechanically ventilated (RR, 0.91; 95% CI, 0.71-1.17) patients with COVID-19. Patients with asthma have a lower risk of death compared with patients without asthma (RR, 0.65; 95% CI, 0.43-0.98). Asthma is not associated with a higher risk of intubation or mechanical ventilation (RR, 1.03; 95% CI, 0.72-1.46).
Conclusions: There is great variability in asthma prevalence among patients with COVID-19 in different countries or regions. Asthma is not associated with higher COVID-19 severity or worse prognosis, and patients with asthma are found to have a lower risk of death compared with patients without asthma.
Keywords: Asthma; COVID-19; Prevalence; Prognosis; Severity.
Copyright © 2020 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- World Health Organization WHO coronavirus disease (COVID-19) dashboard. 2020. https://covid19.who.int Available from:
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
