

Serological evidence indicates widespread distribution of rickettsioses in Myanmar
- PMID: 33310022
- PMCID: PMC7862081
- DOI: 10.1016/j.ijid.2020.12.013
Serological evidence indicates widespread distribution of rickettsioses in Myanmar
Abstract
Background: Little research has been published on the prevalence of rickettsial infections in Myanmar. This study determined the seroprevalence of immunoglobulin G (IgG) antibodies to rickettsial species in different regions of Myanmar.
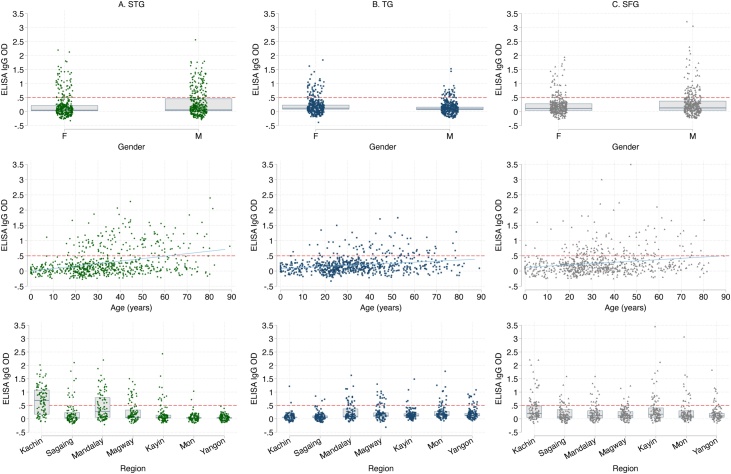
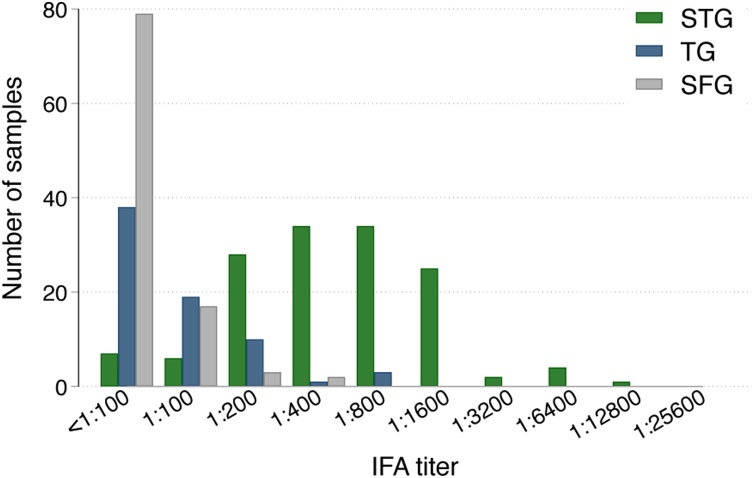
Methods: Seven hundred leftover blood samples from patients of all ages in primary care clinics and hospitals in seven regions of Myanmar were collected. Samples were screened for scrub typhus group (STG), typhus group (TG) and spotted fever group (SFG) IgG antibodies using enzyme-linked immunosorbent assays (ELISA). Immunofluorescence assays were performed for the same rickettsial groups to confirm seropositivity if ELISA optical density ≥0.5.
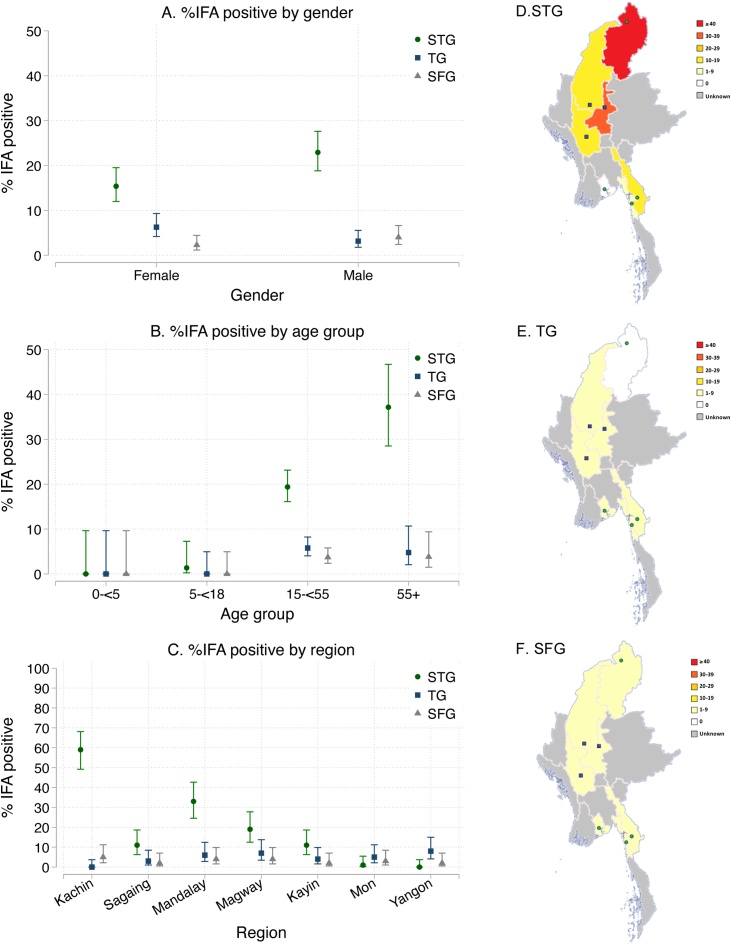
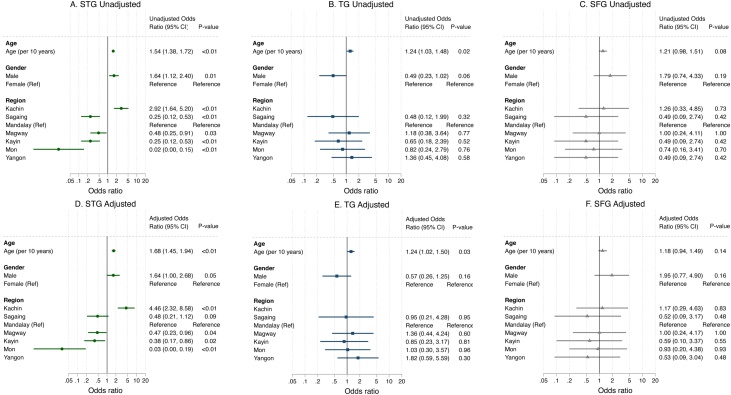
Results: Overall IgG seroprevalence was 19% [95% confidence interval (CI) 16-22%] for STG, 5% (95% CI 3-7%) for TG and 3% (95% CI: 2-5%) for SFG. The seroprevalence of STG was particularly high in northern and central Myanmar (59% and 19-33%, respectively). Increasing age was associated with higher odds of STG and TG seropositivity [per 10-year increase, adjusted odds ratio estimate 1.68 (p < 0.01) and 1.24 (p = 0.03), respectively].
Conclusion: Rickettsial infections are widespread in Myanmar, with particularly high seroprevalence of STG IgG antibodies in central and northern regions. Healthcare workers should consider rickettsial infections as common causes of fever in Myanmar.
Keywords: Murine typhus; Myanmar; Rickettsial infections; Scrub typhus; Seroprevalence; Spotted fever group.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Blacksell S.D., Bryant N.J., Paris D.H., Doust J.A., Sakoda Y., Day N.P.J. Scrub typhus serologic testing with the indirect immunofluorescence method as a diagnostic gold standard: a lack of consensus leads to a lot of confusion. Clin Infect Dis. 2007;44:391–401. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
