

doi: 10.22038/abjs.2020.44481.2224.
Posterior Shoulder Instability: The Augmented McLaughlin Procedure
Affiliations
- PMID: 33313355
- PMCID: PMC7718575
- DOI: 10.22038/abjs.2020.44481.2224
Item in Clipboard
Posterior Shoulder Instability: The Augmented McLaughlin Procedure
Arch Bone Jt Surg.
2020 Nov.
Abstract
Posterior shoulder dislocation, whilst uncommon, is frequently missed and often associated with a significant defect on the antero-medial aspect of the humeral head (the reverse Hill-Sachs lesion). Several techniques for stabilisation have been described, depending on the size of the lesion. We describe an additional technique for stabilising the shoulder following posterior dislocation by augmenting the reverse Hill-Sachs lesion with layers of extracellular matrix, thus further filling the defect.
Keywords: McLaughlin procedure; Posterior dislocation; everse hill-sachs; ll suture anchor; xtracellular matrix.
Figures

Axial view: The subscapularis is peeled from the lesser tuberosity. The long head of biceps (LHB) can be used to orientate the surgeon. Internal rotation may be needed to disengage the humeral head from the acromion

Axial view: Two Iconix, Stryker 2.3mm Double-stranded all suture Anchors are placed in the deepest part of the Hill-Sachs lesion, one superior, one inferior, 1.5-2cm apart. Note figure shows cross section through one anchor

The anchors are placed in the deepest part of the defect. Note stay sutures have been placed in the retracted subscapularis tendon
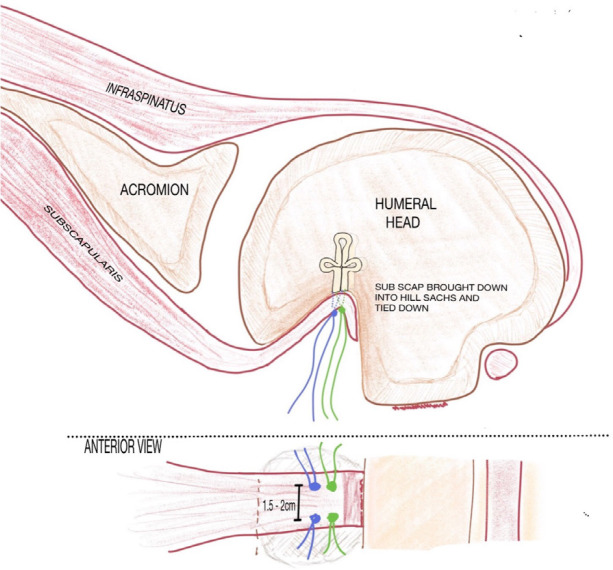
Axial and Anterior View: Each strand of each anchor is passed through the subscapularis tendon and the tendon is snugged down into the defect

Subscapularis is snugged into the defect. Note that the stay sutures in subscapularis have been tied into the rotator cuff laterally

Two patches of ECM (2x1cm) are prepared

Two small holes are made 1.5cm apart in each ECM. Strands from the superior anchor are passed through holes A. Strands from the inferior anchor are passed through holes B

The patches are positioned over defect, superficial to subscapularis

The patches are snugged down into the defect and the strands of the suture anchors are tied over the top of the patches. The suture ends are then shortened

The anchor sutures are tied over the ECM, further filling the defect
References
-
- Cooper A. A Treatise on Dislocations and Fractures of the Joints. Philadelphia: Lea & Blanchard; 1822.
-
- Jacobs RC, Meredyth NA, Mitchelson JD. Easily Missed? Posterior shoulder dislocations. BMJ, 2015:31–32. - PubMed
-
- Cicak N. Posterior dislocation of the shoulder. The Journal of Bone and Joint Surgery. 2004;86(3):324–32. - PubMed
-
- Clyde CT, Throckmorton TW, Duquin TR. Subscapularis Peel in Anatomic Total Shoulder Arthroplasty. Journal of Shoulder and Elbow Arthroplasty. 2018;2(1):1–6.
LinkOut - more resources
Full Text Sources