

Decreased incidence of acute rejection without increased incidence of cytomegalovirus (CMV) infection in kidney transplant recipients receiving rabbit anti-thymocyte globulin without CMV prophylaxis - a cohort single-center study
- PMID: 33314321
- PMCID: PMC8573716
- DOI: 10.1111/tri.13800
Decreased incidence of acute rejection without increased incidence of cytomegalovirus (CMV) infection in kidney transplant recipients receiving rabbit anti-thymocyte globulin without CMV prophylaxis - a cohort single-center study
Abstract
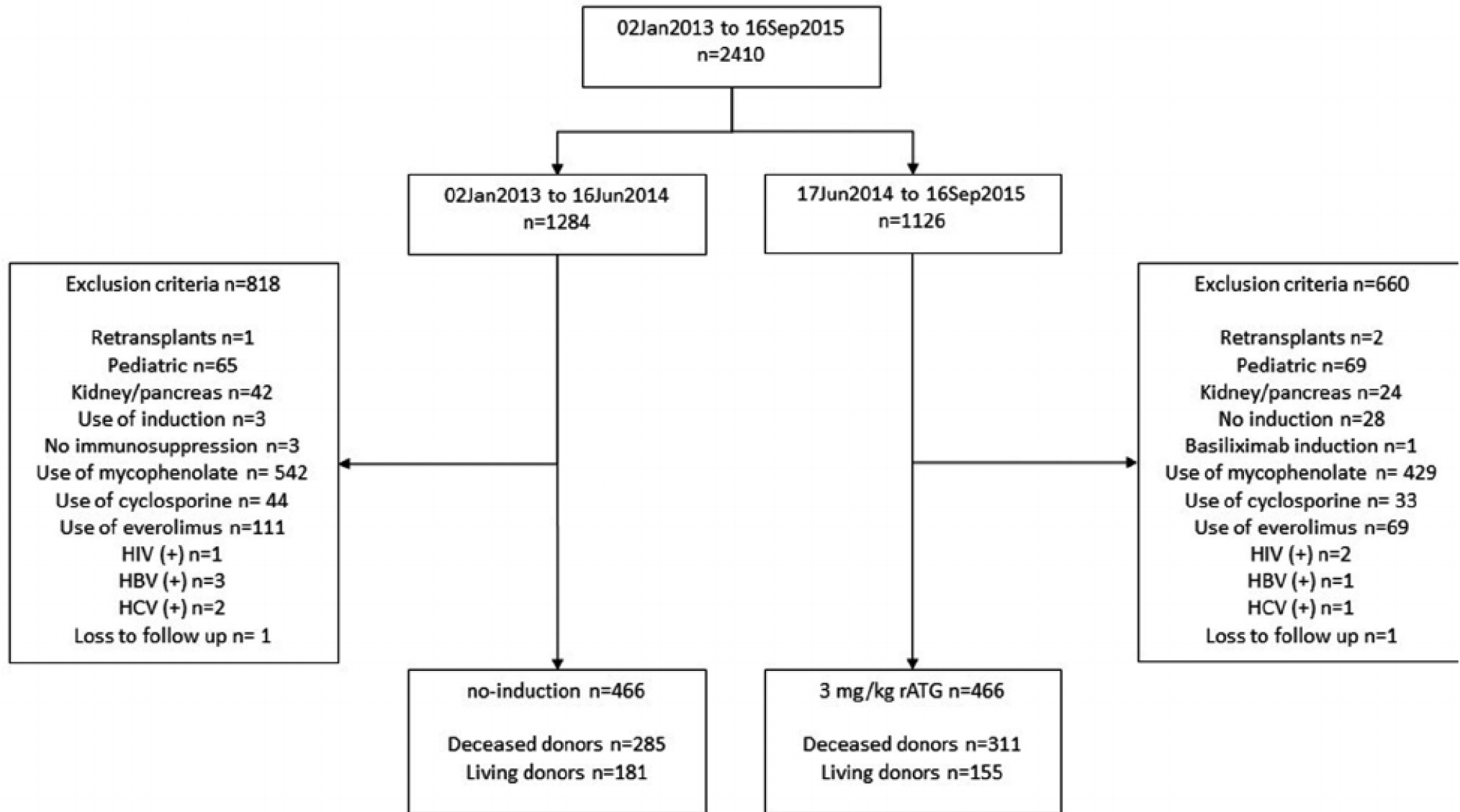
Induction therapy with rabbit anti-thymocyte globulin (rATG) in low-risk kidney transplant recipients (KTR) remains controversial, given the associated increased risk of cytomegalovirus (CMV) infection. This natural experiment compared 12-month clinical outcomes in low-risk KTR without CMV prophylaxis (January/3/13-September/16/15) receiving no induction or a single 3 mg/kg dose of rATG. We used logistic regression to characterize delayed graft function (DGF), negative binomial to characterize length of hospital stay (LOS), and Cox regression to characterize acute rejection (AR), CMV infection, graft loss, death, and hospital readmissions. Recipients receiving 3 mg/kg rATG had an 81% lower risk of AR (aHR 0.14 0.190.25 , P < 0.001) but no increased rate of hospital readmissions because of infections (0.68 0.911.21 , P = 0.5). There was no association between 3 mg/kg rATG and CMV infection/disease (aHR 0.86 1.101.40 , P = 0.5), even when the analysis was stratified according to recipient CMV serostatus positive (aHR 0.94 1.251.65 , P = 0.1) and negative (aHR 0.28 0.571.16 , P = 0.1). There was no association between 3 mg/kg rATG and mortality (aHR 0.51 1.253.08 , P = 0.6), and graft loss (aHR 0.34 0.731.55 , P = 0.4). Among low-risk KTR receiving no CMV pharmacological prophylaxis, 3 mg/kg rATG induction was associated with a significant reduction in the incidence of AR without an increased risk of CMV infection, regardless of recipient pretransplant CMV serostatus.
Keywords: CMV infection; acute rejection; low immunological risk; thymoglobulin.
© 2020 Steunstichting ESOT. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Conflict of interest
The following authors of this manuscript have conflicts of interest to disclose: Helio Tedesco-Silva has received speaker’s fees and travel or accommodation expenses for development of educational presentations and scientific advice from Novartis, Pfizer, and Roche. Jose Medina Pestana has received speaker’s fees and travel or accommodation expenses for development of educational presentations and scientific advice from Bristol-Myers Squibb, Novartis, Pfizer, and Roche. Claudia Felipe has received speaker’s fees for development of educational presentations and travel or accommodation expenses from Novartis and Pfizer. Marina Cristelli has received speaker’s fees for development of educational presentations and travel or accommodation expenses from Novartis and Pfizer. Dorry Segev receives speaking honoraria from Sanofi. The other authors of this manuscript have no conflicts of interest to disclose.
Figures



References
-
- Hardinger KL, Brennan DC, Klein CL. Selection of induction therapy in kidney transplantation. Transpl Int 2013; 26: 662. - PubMed
-
- Kidney Disease: Improving Global Outcomes Transplant Work G. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant 2009; 9 (Suppl 3): S1. - PubMed
-
- Hiramoto LL, Tedesco-Silva H, Medina-Pestana JO, Felipe CR. Tolerability of mycophenolate sodium in renal transplant recipients. Int J Clin Pharm 2018; 40: 1548. - PubMed
-
- de Paula MI, Bae S, Shaffer AA, et al. The influence of antithymocyte globulin dose on the incidence of CMV infection in high-risk kidney transplant recipients without pharmacological prophylaxis. Transplantation 2020; 104: 2139. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
