

Predictive Biomarkers for Immune Checkpoint Inhibitors in Metastatic Breast Cancer
- PMID: 33314633
- PMCID: PMC7826457
- DOI: 10.1002/cam4.3550
Predictive Biomarkers for Immune Checkpoint Inhibitors in Metastatic Breast Cancer
Abstract
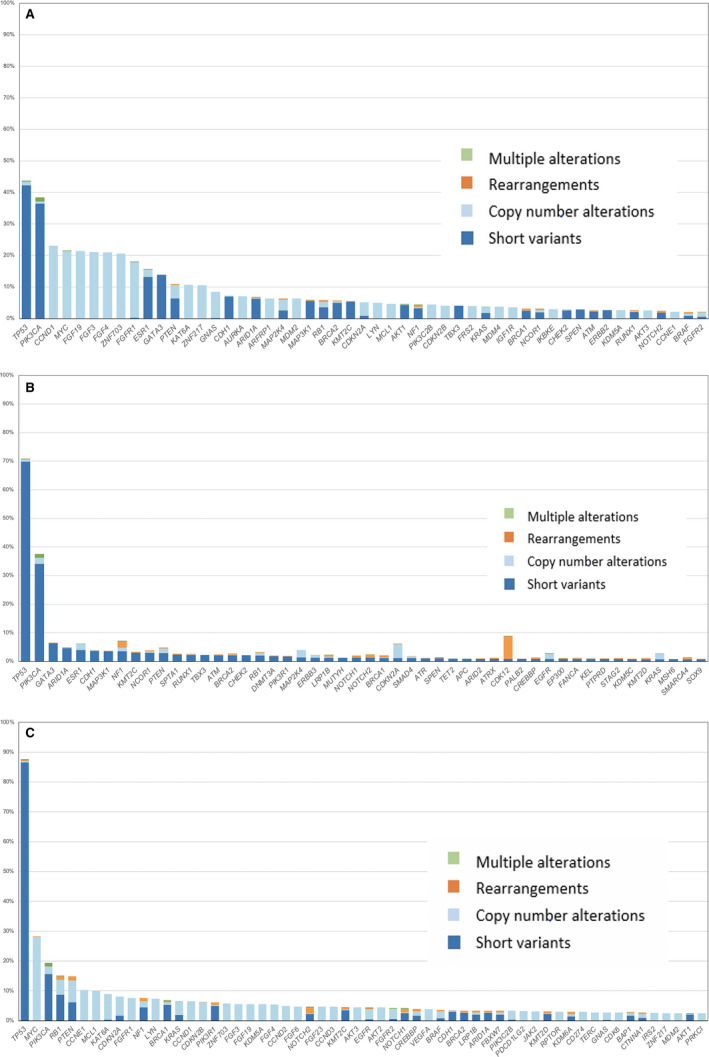
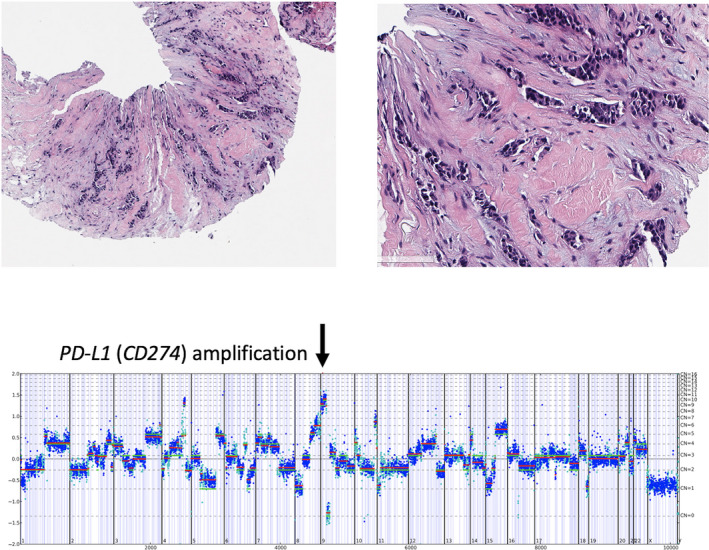
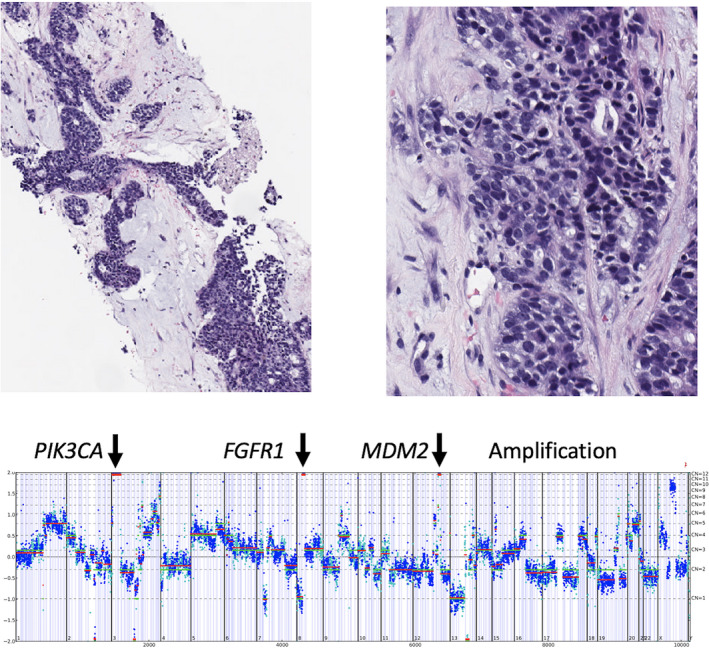
We examined a large dataset of female metastatic breast cancers (MBCs) profiled with comprehensive genomic profiling (CGP) to identify the prevalence and distribution of immunotherapy responsiveness-associated biomarkers. DNA was extracted from 3831 consecutive MBCs: 1237 (ERpos /HER2neg ), 1953 ERneg /HER2amp , and 641 triple-negative breast cancer (TNBC). CGP was performed using the FoundationOne® or FoundationOne® CDx NGS assay. Tumor mutational burden (TMB) and microsatellite instability (MSI) were determined in a subset of cases. PD-L1 expression in immunocytes in a subset of cases was determined by immunohistochemistry using the companion diagnostic VENTANA PD-L1 SP142 Assay. The median age of the cohort was 54 years (range 20-89). Genomic alterations (GAs)/tumor were similar (range: 5.9-7.3). Markers of potential immune checkpoint inhibitor (ICPI) benefit included: CD274 (PD-L1) amplification (1%-3%), BRAF GA (1%-4%), TMB of ≥10 mutations/Mb (8%-12%), MSI-high (0.1%-0.4%), PBRM1 GA (1%), and positive PD-L1 staining of immunocytes ranging from 13% in ERpos /HER2neg and 33% in ERneg /HER2amp to 47% in the TNBC group. Potential markers of ICPI resistance included inactivating STK11 GA (1%-2%) and MDM2 amplification (3%-6%). MTOR pathway targets were common with lowest frequency in TNBC. ERBB2 short variant mutations were most frequent ERpos /HER2neg and absent in TNBC. BRCA1/2 GA were least frequent in ERneg /HER2amp . The demonstrations of clinical benefit of immunotherapy in MBC support the need for development and utilization of biomarkers to guide the use of ICPIs for these patients. In addition to guiding therapy selection, CGP shows potential to identify GA linked to response and resistance to ICPI in MBC.
Keywords: PD-L1; biomarkers; comprehensive genomic profiling; immunotherapy; metastatic breast cancer; microsatellite instability; tumor mutational burden.
© 2020 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Abirami Sivapiragasam: No conflict to disclose. P. Ashok Kumar: No conflict to disclose. Ethan S. Sokol: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Lee A. Albacker: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd, J. Keith Killian: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Shakti Ramkissoon: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Richard Huang: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Patents with VENTANA (Roche). Eric A. Severson: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Natalie Danziger: Employment by Foundation Medicine Inc. Charlotte A. Brown: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Kimberly McGregor: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd. Jeffrey S. Ross: Employment by Foundation Medicine Inc. Stock in F. Hoffman La Roche Ltd.
Figures
References
-
- Hargadon KM, Johnson CE, Williams CJ. Immune checkpoint blockade therapy for cancer: an overview of FDA‐approved immune checkpoint inhibitors. Int Immunopharmacol. 2018;62:29‐39. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
