

Effectiveness of Mindfulness Meditation vs Headache Education for Adults With Migraine: A Randomized Clinical Trial
- PMID: 33315046
- PMCID: PMC7737157
- DOI: 10.1001/jamainternmed.2020.7090
Effectiveness of Mindfulness Meditation vs Headache Education for Adults With Migraine: A Randomized Clinical Trial
Abstract
Importance: Migraine is the second leading cause of disability worldwide. Most patients with migraine discontinue medications due to inefficacy or adverse effects. Mindfulness-based stress reduction (MBSR) may provide benefit.
Objective: To determine if MBSR improves migraine outcomes and affective/cognitive processes compared with headache education.
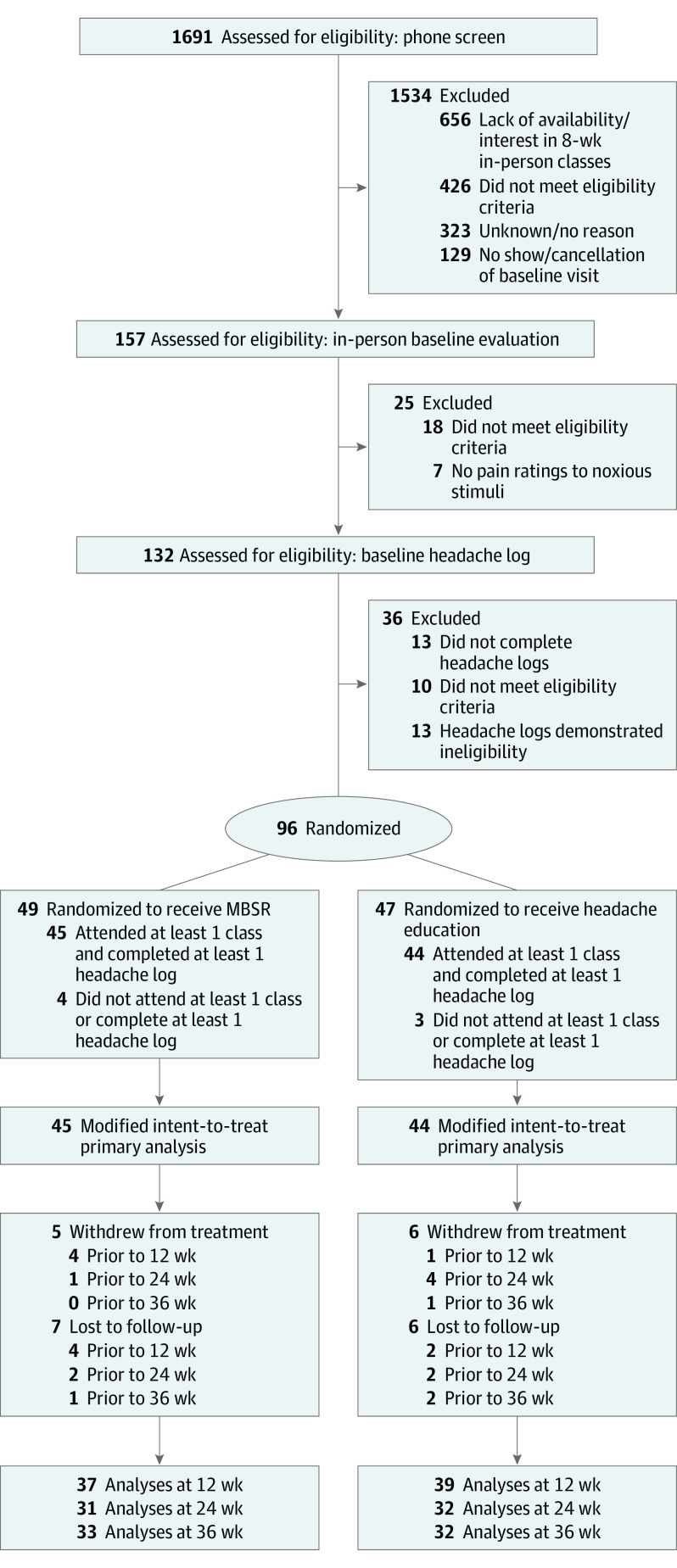
Design, setting, and participants: This randomized clinical trial of MBSR vs headache education included 89 adults who experienced between 4 and 20 migraine days per month. There was blinding of participants (to active vs comparator group assignments) and principal investigators/data analysts (to group assignment).
Interventions: Participants underwent MBSR (standardized training in mindfulness/yoga) or headache education (migraine information) delivered in groups that met for 2 hours each week for 8 weeks.
Main outcomes and measures: The primary outcome was change in migraine day frequency (baseline to 12 weeks). Secondary outcomes were changes in disability, quality of life, self-efficacy, pain catastrophizing, depression scores, and experimentally induced pain intensity and unpleasantness (baseline to 12, 24, and 36 weeks).
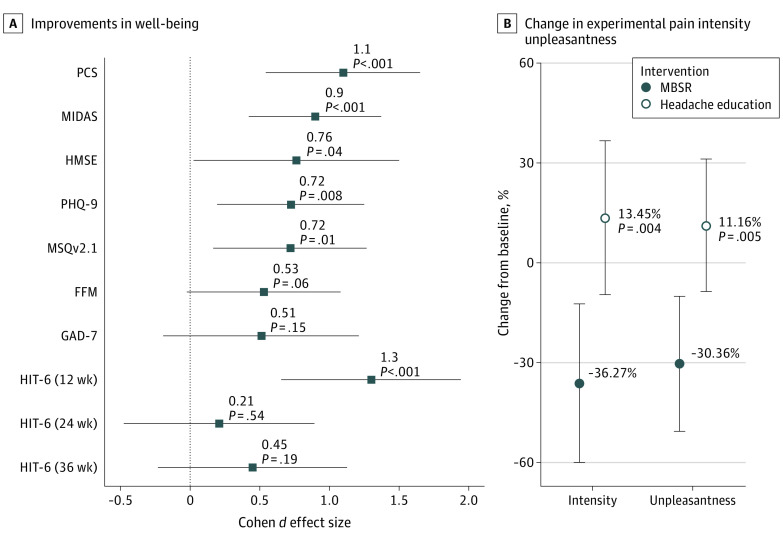
Results: Most participants were female (n = 82, 92%), with a mean (SD) age of 43.9 (13.0) years, and had a mean (SD) of 7.3 (2.7) migraine days per month and high disability (Headache Impact Test-6: 63.5 [5.7]), attended class (median attendance, 7 of 8 classes), and followed up through 36 weeks (33 of 45 [73%] of the MBSR group and 32 of 44 [73%] of the headache education group). Participants in both groups had fewer migraine days at 12 weeks (MBSR: -1.6 migraine days per month; 95% CI, -0.7 to -2.5; headache education: -2.0 migraine days per month; 95% CI, -1.1 to -2.9), without group differences (P = .50). Compared with those who participated in headache education, those who participated in MBSR had improvements from baseline at all follow-up time points (reported in terms of point estimates of effect differences between groups) on measures of disability (5.92; 95% CI, 2.8-9.0; P < .001), quality of life (5.1; 95% CI, 1.2-8.9; P = .01), self-efficacy (8.2; 95% CI, 0.3-16.1; P = .04), pain catastrophizing (5.8; 95% CI, 2.9-8.8; P < .001), depression scores (1.6; 95% CI, 0.4-2.7; P = .008), and decreased experimentally induced pain intensity and unpleasantness (MBSR group: 36.3% [95% CI, 12.3% to 60.3%] decrease in intensity and 30.4% [95% CI, 9.9% to 49.4%] decrease in unpleasantness; headache education group: 13.5% [95% CI, -9.9% to 36.8%] increase in intensity and an 11.2% [95% CI, -8.9% to 31.2%] increase in unpleasantness; P = .004 for intensity and .005 for unpleasantness, at 36 weeks). One reported adverse event was deemed unrelated to study protocol.
Conclusions and relevance: Mindfulness-based stress reduction did not improve migraine frequency more than headache education, as both groups had similar decreases; however, MBSR improved disability, quality of life, self-efficacy, pain catastrophizing, and depression out to 36 weeks, with decreased experimentally induced pain suggesting a potential shift in pain appraisal. In conclusion, MBSR may help treat total migraine burden, but a larger, more definitive study is needed to further investigate these results.
Trial registration: ClinicalTrials.gov Identifier: NCT02695498.
Conflict of interest statement
Figures

Comment in
-
Are Methods for Evaluating Medications Appropriate for Evaluating Nonpharmacological Treatments for Pain?-Challenges for an Emerging Field of Research.JAMA Intern Med. 2021 Mar 1;181(3):328-329. doi: 10.1001/jamainternmed.2020.7081. JAMA Intern Med. 2021. PMID: 33315054 No abstract available.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. doi: 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Archibald N, Lipscomb J, McCrory DC. Resource Utilization and Costs of Care for Treatment of Chronic Headache. In: AHRQ Technical Reviews and Summaries. US Agency for Health Care Policy and Research; 1999. - PubMed
-
- Loder E, Weizenbaum E, Frishberg B, Silberstein S; American Headache Society Choosing Wisely Task Force . Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question. Headache. 2013;53(10):1651-1659. doi: 10.1111/head.12233 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
