

Assessment of Electronic Health Record Use Between US and Non-US Health Systems
- PMID: 33315048
- PMCID: PMC7737152
- DOI: 10.1001/jamainternmed.2020.7071
Assessment of Electronic Health Record Use Between US and Non-US Health Systems
Erratum in
-
Omission in the Author Contributions Section.JAMA Intern Med. 2021 Feb 1;181(2):296. doi: 10.1001/jamainternmed.2020.8964. JAMA Intern Med. 2021. PMID: 33523124 Free PMC article. No abstract available.
Abstract
Importance: Understanding how the electronic health record (EHR) system changes clinician work, productivity, and well-being is critical. Little is known regarding global variation in patterns of use.
Objective: To provide insights into which EHR activities clinicians spend their time doing, the EHR tools they use, the system messages they receive, and the amount of time they spend using the EHR after hours.
Design, setting, and participants: This cross-sectional study analyzed the deidentified metadata of ambulatory care health systems in the US, Canada, Northern Europe, Western Europe, the Middle East, and Oceania from January 1, 2019, to August 31, 2019. All of these organizations used the EHR software from Epic Systems and represented most of Epic Systems's ambulatory customer base. The sample included all clinicians with scheduled patient appointments, such as physicians and advanced practice practitioners.
Exposures: Clinician EHR use was tracked by deidentified and aggregated metadata across a variety of clinical activities.
Main outcomes and measures: Descriptive statistics for clinician EHR use included time spent on clinical activities, note documentation (as measured by the percentage of characters in the note generated by automated or manual data entry source), messages received, and time spent after hours.
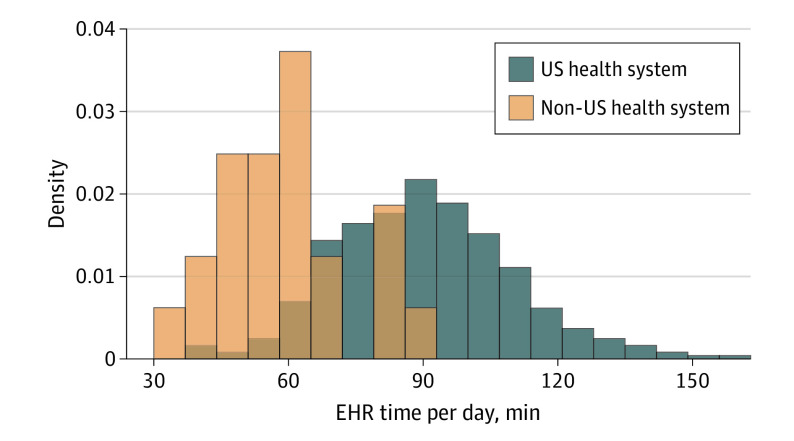
Results: A total of 371 health systems were included in the sample, of which 348 (93.8%) were located in the US and 23 (6.2%) were located in other countries. US clinicians spent more time per day actively using the EHR compared with non-US clinicians (mean time, 90.2 minutes vs 59.1 minutes; P < .001). In addition, US clinicians vs non-US clinicians spent significantly more time performing 4 clinical activities: notes (40.7 minutes vs 30.7 minutes; P < .001), orders (19.5 minutes vs 8.75 minutes; P < .001), in-basket messages (12.5 minutes vs 4.80 minutes; P < .001), and clinical review (17.6 minutes vs 14.8 minutes; P = .01). Clinicians in the US composed more automated note text than their non-US counterparts (77.5% vs 60.8% of note text; P < .001) and received statistically significantly more messages per day (33.8 vs 12.8; P < .001). Furthermore, US clinicians used the EHR for a longer time after hours, logging in 26.5 minutes per day vs 19.5 minutes per day for non-US clinicians (P = .01). The median US clinician spent as much time actively using the EHR per day (90.1 minutes) as a non-US clinician in the 99th percentile of active EHR use time per day (90.7 minutes) in the sample. These results persisted after controlling for organizational characteristics, including structure, type, size, and daily patient volume.
Conclusions and relevance: This study found that US clinicians compared with their non-US counterparts spent substantially more time actively using the EHR for a wide range of clinical activities or tasks. This finding suggests that US clinicians have a greater EHR burden that may be associated with nontechnical factors, which policy makers and health system leaders should consider when addressing clinician wellness.
Conflict of interest statement
Figures

Comment in
-
Advancing Practice Science With Electronic Health Record Use Data.JAMA Intern Med. 2021 Feb 1;181(2):260-261. doi: 10.1001/jamainternmed.2020.7068. JAMA Intern Med. 2021. PMID: 33315045 No abstract available.
References
-
- Centers for Medicare & Medicaid Services Promoting interoperability (Pl) program. Published October 2018. Accessed June 8, 2020. https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePro...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
