

Characteristics, comorbidities and survival analysis of young adults hospitalized with COVID-19 in New York City
- PMID: 33315929
- PMCID: PMC7735602
- DOI: 10.1371/journal.pone.0243343
Characteristics, comorbidities and survival analysis of young adults hospitalized with COVID-19 in New York City
Abstract
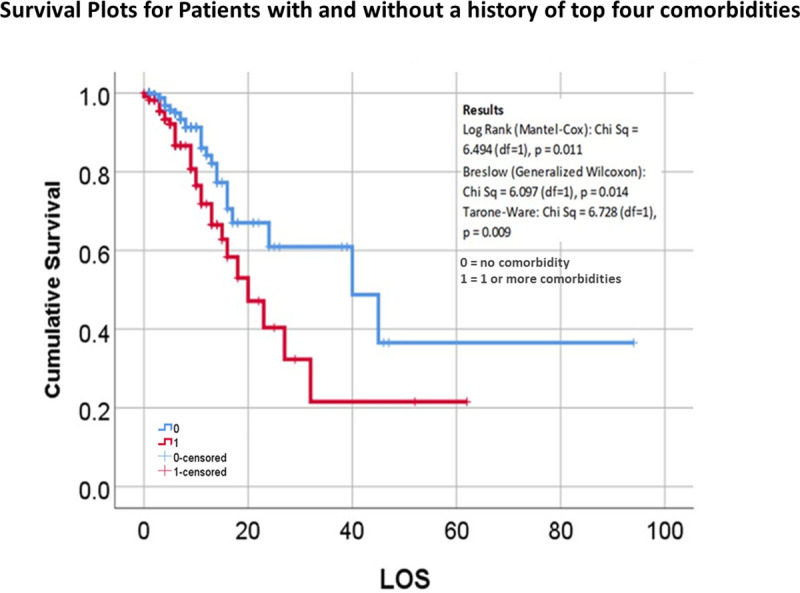
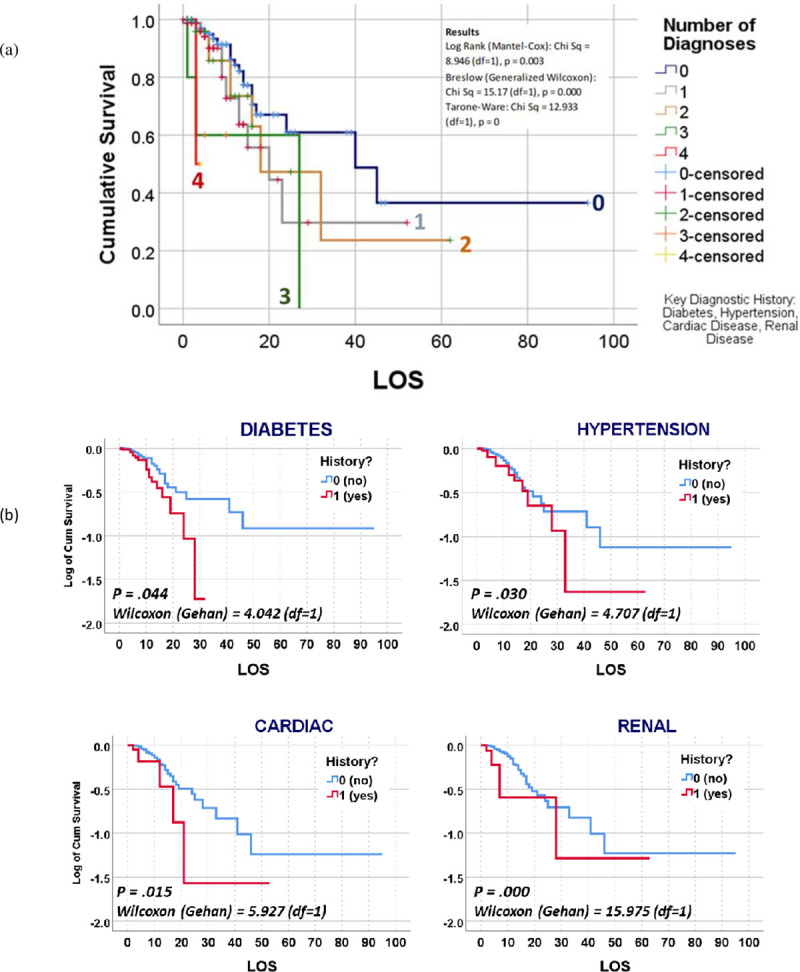
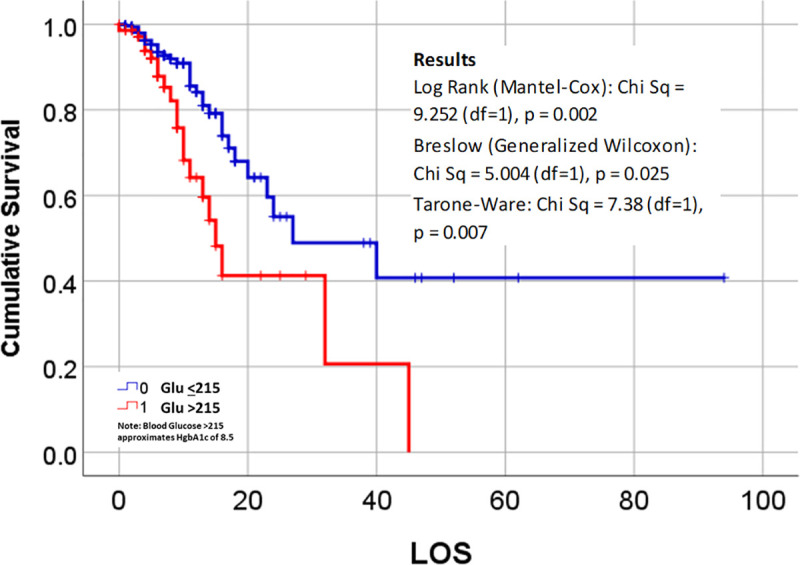
This study reviewed 395 young adults, 18-35 year-old, admitted for COVID-19 to one of the eleven hospitals in New York City public health system. Demographics, comorbidities, clinical course, outcomes and characteristics linked to hospitalization were analyzed including temporal survival analysis. Fifty-seven percent of patients had a least one major comorbidity. Mortality without comorbidity was in 3.8% patients. Further investigation of admission features and medical history was conducted. Comorbidities associated with mortality were diabetes (n = 54 deceased/73 diagnosed,74% tested POS;98.2% with diabetic history deceased; Wilcoxon p (Wp) = .044), hypertension (14/44,32% POS, 25.5%; Wp = 0.030), renal (6/16, 37.5% POS,11%; Wp = 0.000), and cardiac (6/21, 28.6% POS,11%; Wp = 0.015). Kaplan survival plots were statistically significant for these four indicators. Data suggested glucose >215 or hemoglobin A1c >9.5 for young adults on admission was associated with increased mortality. Clinically documented respiratory distress on admission was statistically significant outcome related to mortality (X2 = 236.6842, df = 1, p < .0001). Overall, 28.9% required supportive oxygen beyond nasal cannula. Nasal cannula oxygen alone was required for 71.1%, who all lived. Non-invasive ventilation was required for 7.8%, and invasive mechanical ventilation 21.0% (in which 7.3% lived, 13.7% died). Temporal survival analysis demonstrated statistically significant response for Time to Death <10 days (X2 = 18.508, df = 1, p = .000); risk lessened considerably for 21 day cut off (X2 = 3.464, df = 1, p = .063), followed by 31 or more days of hospitalization (X2 = 2.212, df = 1, p = .137).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
