

Erenumab for headaches in idiopathic intracranial hypertension: A prospective open-label evaluation
- PMID: 33316102
- PMCID: PMC7898289
- DOI: 10.1111/head.14026
Erenumab for headaches in idiopathic intracranial hypertension: A prospective open-label evaluation
Abstract
Objective: To determine the effectiveness of erenumab in treating headaches in idiopathic intracranial hypertension (IIH) in whom papilledema had resolved.
Background: Disability in IIH is predominantly driven by debilitating headaches with no evidence for the use of preventative therapies. Headache therapy in IIH is an urgent unmet need.
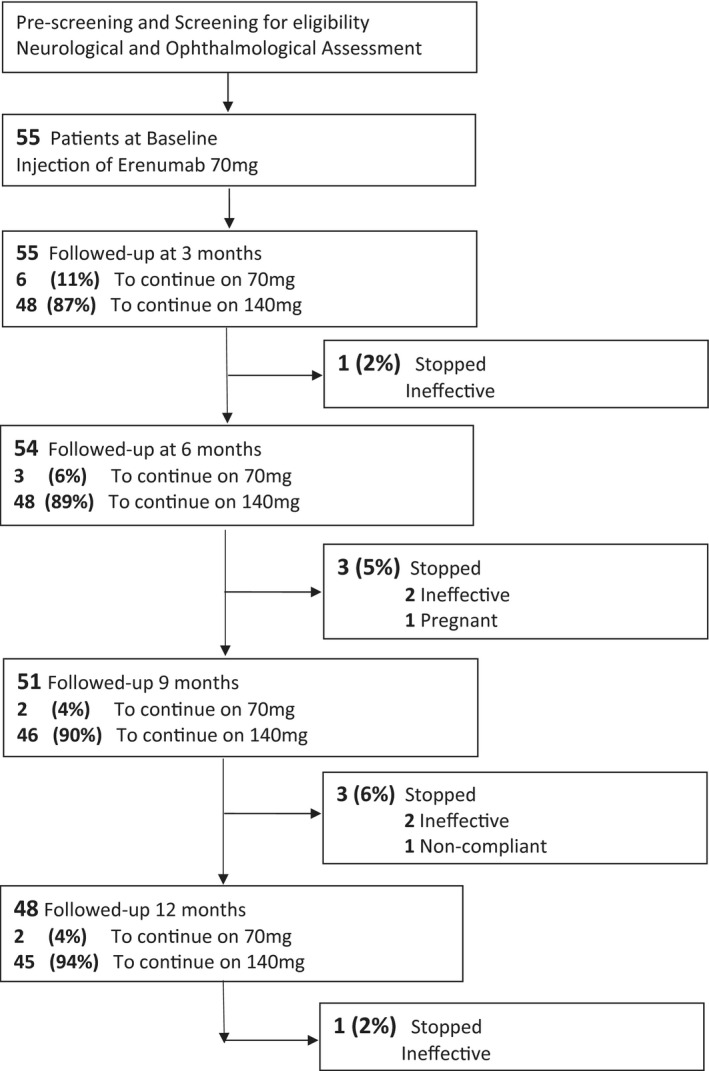
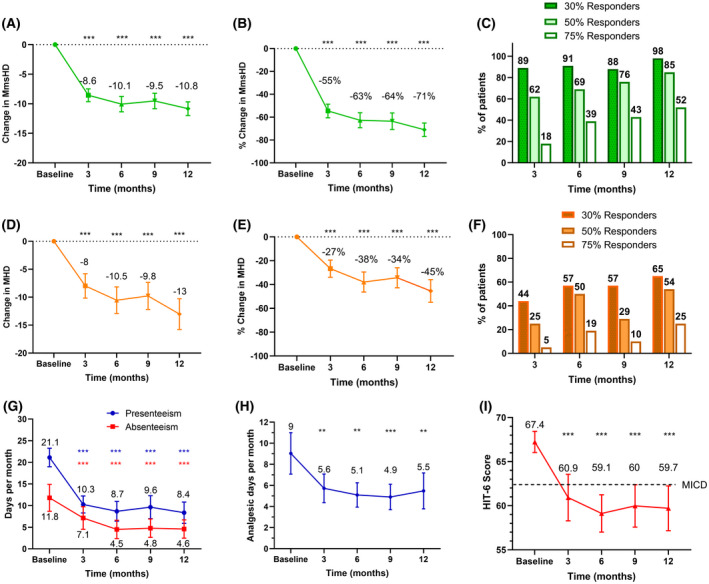
Methods: A prospective, open-label study in the United Kingdom was conducted. Adult females with confirmed diagnosis of IIH now in ocular remission (papilledema resolved) with chronic headaches (≥15 days a month) and failure of ≥3 preventative medications received erenumab 4-weekly (assessments were 3-monthly). The primary end point was change in monthly moderate/severe headache days (MmsHD) from baseline (30-day pretreatment period) compared to 12 months.
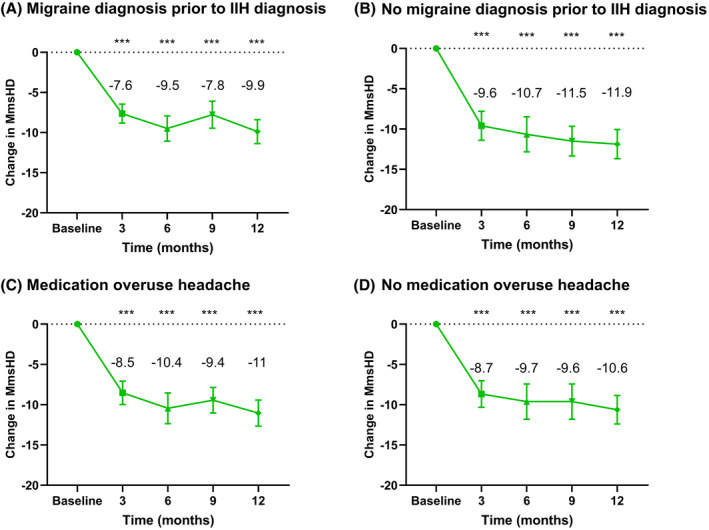
Results: Fifty-five patients, mean (SD) age 35.3 (9) years and mean duration of headaches 10.4 (8.4) years with 3.7 (0.9) preventative treatment failures, were enrolled. Mean baseline MmsHD was 16.1 (4.7) and total monthly headache days (MHD) was (29) 2.3. MmsHD reduced substantially at 12 months by mean (SD) [95% CI] 10.8 (4.0) [9.5, 11.9], p < 0.001 and MHD reduced by 13.0 (9.5) [10.2, 15.7], p < 0.001. Crystal clear days (days without any head pain) increased by 13.1 (9.5) [9.6, 15.3], p < 0.001, headache severity (scale 0-10) fell by 1.3 (1.7) [0.9, 1.9], p < 0.001, and monthly analgesic days reduced by 4.3 (9.2) [1.6, 6.9], p = 0.002. All these measures had improved significantly by 3 months, with a consistent significant response to 12 months. Headache impact test-6 score and quality of life Short Form-36 Health Survey significantly improved at 12 months. Sensitivity analysis revealed similar results for patients with and without a prior migraine diagnosis (28/55 (52%) patients) or those with or without medication overuse (27/55 (48%) patients).
Conclusions: This study provides evidence for the effectiveness of erenumab to treat headaches in IIH patients with resolution of papilledema. It provides mechanistic insights suggesting that calcitonin gene-related peptide is likely a modulator driving headache and a useful therapeutic target.
Keywords: calcitonin gene-related peptide monoclonal antibody; headache; idiopathic intracranial hypertension; papilledema; raised intracranial pressure.
© 2020 The Authors. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Yiangou, Mitchell, Fisher, Vijay, Alimajstorovic, Lavery declare no conflict. Edwards has received speaker fees and Honoria from Novartis, Teva, Eli Lily, and Allergan on headache treatments but not related to IIH. Mollan has received Honoria from Novartis for speaking on topics unrelated to this drug, but within a National headache network meeting (November 2019). Sinclair has received speaker fees and Honoraria from Novartis (erenumab) and Allergan (BOTOX), in addition, Invex therapeutics, company director with salary and stock options (2019, 2020). Grech has received fees for consultancy work for Invex therapeutics (2020). The authors declare no other financial relationships with any organizations that might have an interest in the submitted work; and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
