

HIV infection and COVID-19 death: a population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform
- PMID: 33316211
- PMCID: PMC7773630
- DOI: 10.1016/S2352-3018(20)30305-2
HIV infection and COVID-19 death: a population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform
Abstract
Background: Whether HIV infection is associated with risk of death due to COVID-19 is unclear. We aimed to investigate this association in a large-scale population-based study in England.
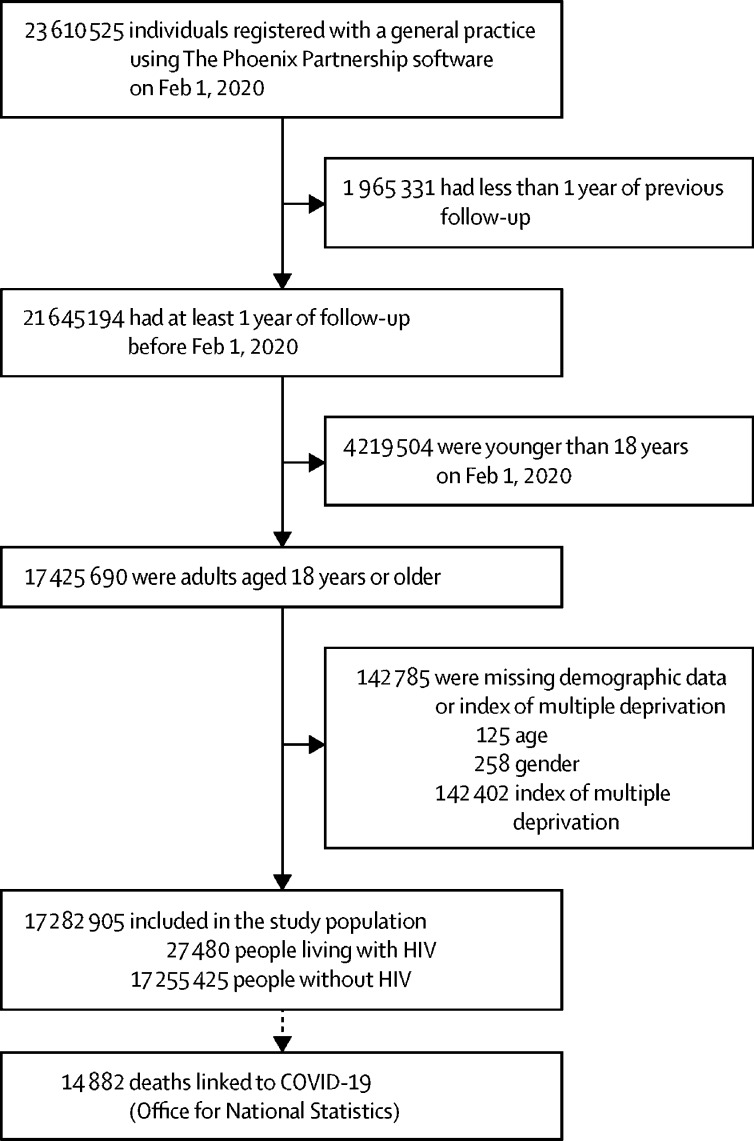
Methods: We did a retrospective cohort study. Working on behalf of NHS England, we used the OpenSAFELY platform to analyse routinely collected electronic primary care data linked to national death registrations. We included all adults (aged ≥18 years) alive and in follow-up on Feb 1, 2020, and with at least 1 year of continuous registration with a general practitioner before this date. People with a primary care record for HIV infection were compared with people without HIV. The outcome was COVID-19 death, defined as the presence of International Classification of Diseases 10 codes U07.1 or U07.2 anywhere on the death certificate. Cox regression models were used to estimate the association between HIV infection and COVID-19 death; they were initially adjusted for age and sex, then we added adjustment for index of multiple deprivation and ethnicity, and then for a broad range of comorbidities. Interaction terms were added to assess effect modification by age, sex, ethnicity, comorbidities, and calendar time.
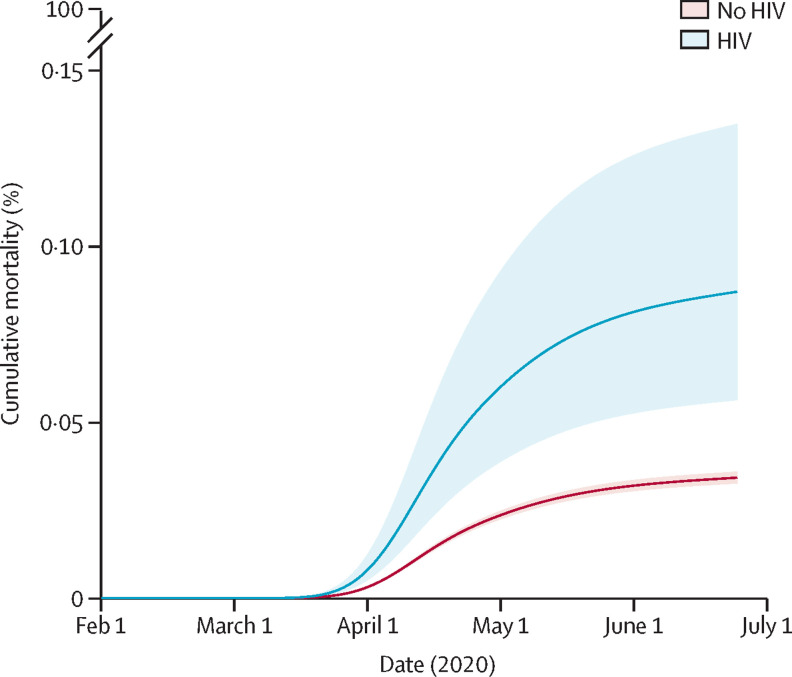
Results: 17 282 905 adults were included, of whom 27 480 (0·16%) had HIV recorded. People living with HIV were more likely to be male, of Black ethnicity, and from a more deprived geographical area than the general population. 14 882 COVID-19 deaths occurred during the study period, with 25 among people with HIV. People living with HIV had higher risk of COVID-19 death than those without HIV after adjusting for age and sex: hazard ratio (HR) 2·90 (95% CI 1·96-4·30; p<0·0001). The association was attenuated, but risk remained high, after adjustment for deprivation, ethnicity, smoking and obesity: adjusted HR 2·59 (95% CI 1·74-3·84; p<0·0001). There was some evidence that the association was larger among people of Black ethnicity: HR 4·31 (95% CI 2·42-7·65) versus 1·84 (1·03-3·26) in non-Black individuals (p-interaction=0·044).
Interpretation: People with HIV in the UK seem to be at increased risk of COVID-19 mortality. Targeted policies should be considered to address this raised risk as the pandemic response evolves.
Funding: Wellcome, Royal Society, National Institute for Health Research, National Institute for Health Research Oxford Biomedical Research Centre, UK Medical Research Council, Health Data Research UK.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
COVID-19 death in people with HIV: interpret cautiously.Lancet HIV. 2021 Jan;8(1):e2-e3. doi: 10.1016/S2352-3018(20)30332-5. Epub 2020 Dec 11. Lancet HIV. 2021. PMID: 33316210 Free PMC article. No abstract available.
References
-
- European Centre for Disease Prevention and Control . European Centre for Disease Prevention and Control; 2020. COVID-19 situation update worldwide, as of 26 November 2020.https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases
-
- Neuzil KM, Reed GW, Mitchel EF, Jr, Griffin MR. Influenza-associated morbidity and mortality in young and middle-aged women. JAMA. 1999;281:901–907. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
