

Optimizing the management of intermediate-stage hepatocellular carcinoma: Current trends and prospects
- PMID: 33317248
- PMCID: PMC8046626
- DOI: 10.3350/cmh.2020.0204
Optimizing the management of intermediate-stage hepatocellular carcinoma: Current trends and prospects
Abstract
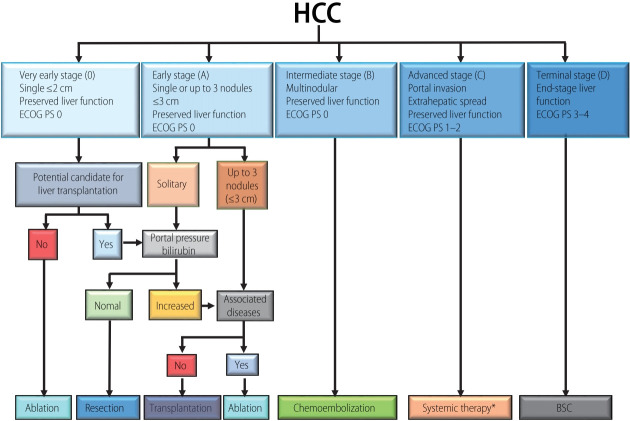
Hepatocellular carcinoma (HCC) is usually accompanied by chronic liver damage, which sometimes influences the selection of HCC treatment. The Barcelona Clinic Liver Cancer (BCLC) staging system, which was first introduced in 1999, is the most commonly used worldwide. Although the intermediate-stage (BCLC stage B) includes the largest number and heterogeneous HCC patients, the recommended treatment option is transarterial chemoembolization (TACE) only. However, recent progress in radical treatments such as hepatic resection, liver transplantation, radiation therapy, and percutaneous therapy has made it possible to treat selected patients with BCLC stage B HCC. Radical treatments are expected to prolong survival time. To-date, TACE has also progressed. In addition to conventional TACE, balloon-occluded TACE and drug-eluting beads TACE are available. These new modalities of TACE will improve therapeutic efficacy and reduce adverse events. One of the most serious concerns of TACE is that repeated TACE reduces the treatment effect and induces liver function impairment. The decision on when TACE should be interrupted is complex. Many molecular targeted agents are now available, and immune checkpoint inhibitors will soon be available for HCC patients with Child-Pugh class A worldwide. Under these circumstances, in patients with TACE unsuitability, switching to molecular targeted agents before deterioration of liver function might improve the prognosis compared to repeated TACE. We should pay attention to stop TACE in TACE-unsuitable HCC patients as it can induce the deterioration of liver function.
Keywords: BCLC; Carcinoma, Hepatocellular; Chemoembolization, Therapeutic; Immune checkpoint inhibitors; Molecular targeted therapy.
Conflict of interest statement
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380:1450–1462. - PubMed
-
- Yin L, Li H, Li AJ, Lau WY, Pan ZY, Lai EC, et al. Partial hepatectomy vs. transcatheter arterial chemoembolization for resectable multiple hepatocellular carcinoma beyond Milan criteria: a RCT. J Hepatol. 2014;61:82–88. - PubMed
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–390. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
