

Relationship between angiography timing and angiographic visualization of extravasation in patients with acute non-variceal gastrointestinal bleeding
- PMID: 33317472
- PMCID: PMC7737270
- DOI: 10.1186/s12876-020-01570-y
Relationship between angiography timing and angiographic visualization of extravasation in patients with acute non-variceal gastrointestinal bleeding
Abstract
Background: Angiographic embolization is now considered the first-line therapy for acute gastrointestinal (GI) bleeding refractory to endoscopic therapy. The success of angiographic embolization depends on the detection of the bleeding site. This study aimed to identify the clinical and procedural predictors for the angiographic visualization of extravasation, including angiography timing, as well as analyze the outcomes of angiographic embolization according to the angiographic visualization of extravasation.
Methods: The clinical and procedural data of 138 consecutive patients (mean age, 66.5 years; 65.9% men) who underwent angiography with or without embolization for acute non-variceal GI bleeding between February 2008 and July 2018 were retrospectively analyzed.
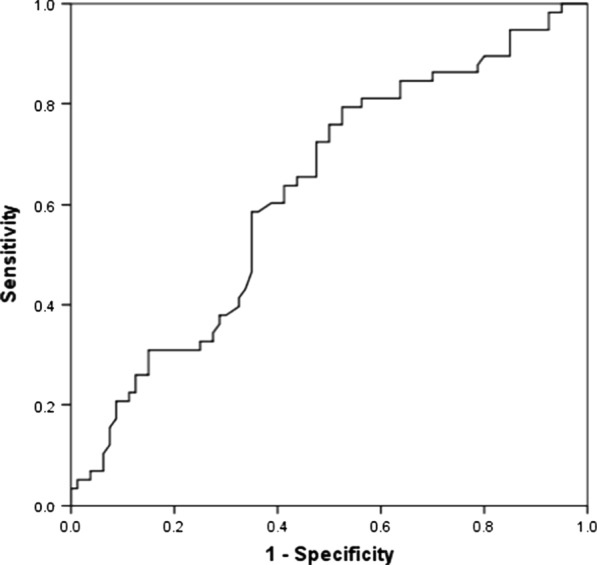
Results: Of the 138 patients, 58 (42%) had active extravasation on initial angiography and 113 (81.9%) underwent embolization. The angiographic visualization of extravasation was significantly higher in patients with diabetes (p = 0.036), a low platelet count (p = 0.048), high maximum heart rate (p = 0.002) and AIMS65 score (p = 0.026), upper GI bleeding (p = 0.025), and short time-to-angiography (p = 0.031). The angiographic embolization was successful in all angiograms, with angiographic visualization of extravasation (100%). The clinical success of patients without angiographic visualization of extravasation (83.9%) was significantly higher than that of patients with angiographic visualization of extravasation (65.5%) (p = 0.004). In multivariate analysis, the time-to-angiography (odds ratio 0.373 [95% CI 0.154-0.903], p = 0.029) was the only significant predictor associated with the angiographic visualization of extravasation. The cutoff value of time-to-angiography was 5.0 h, with a sensitivity and specificity of 79.3% and 47.5%, respectively (p = 0.012).
Conclusions: Angiography timing is an important factor that is associated with the angiographic visualization of extravasation in patients with acute GI bleeding. Angiography should be performed early in the course of bleeding in critically ill patients.
Keywords: Angiography; Endovascular; Gastrointestinal bleeding; Trans-arterial embolization.
Conflict of interest statement
We declare that we do not have any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
Figures


References
-
- van Leerdam ME, Vreeburg EM, Rauws EA, Geraedts AA, Tijssen JG, Reitsma JB, Tytgat GN. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003;98(7):1494–1499. doi: 10.1111/j.1572-0241.2003.07517.x. - DOI - PubMed
-
- Prakash C, Zuckerman GR. Acute small bowel bleeding: a distinct entity with significantly different economic implications compared with GI bleeding from other locations. Gastrointest Endosc. 2003;58(3):330–335. - PubMed
-
- Sanders DS, Perry MJ, Jones SG, McFarlane E, Johnson AG, Gleeson DC, Lobo AJ. Effectiveness of an upper-gastrointestinal haemorrhage unit: a prospective analysis of 900 consecutive cases using the Rockall score as a method of risk standardisation. Eur J Gastroenterol Hepatol. 2004;16(5):487–494. doi: 10.1097/00042737-200405000-00009. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
