

High flow nasal therapy versus noninvasive ventilation as initial ventilatory strategy in COPD exacerbation: a multicenter non-inferiority randomized trial
- PMID: 33317579
- PMCID: PMC7734463
- DOI: 10.1186/s13054-020-03409-0
High flow nasal therapy versus noninvasive ventilation as initial ventilatory strategy in COPD exacerbation: a multicenter non-inferiority randomized trial
Abstract
Background: The efficacy and safety of high flow nasal therapy (HFNT) in patients with acute hypercapnic exacerbation of chronic obstructive pulmonary disease (AECOPD) are unclear. Our aim was to evaluate the short-term effect of HFNT versus NIV in patients with mild-to-moderate AECOPD, with the hypothesis that HFNT is non-inferior to NIV on CO2 clearance after 2 h of treatment.
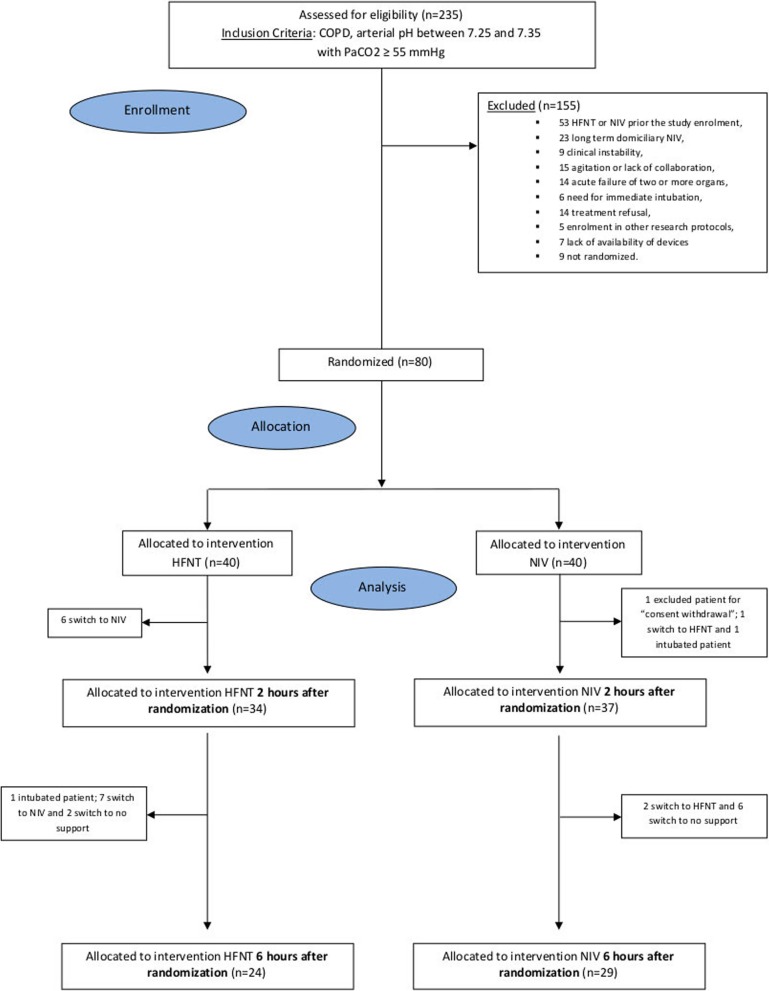
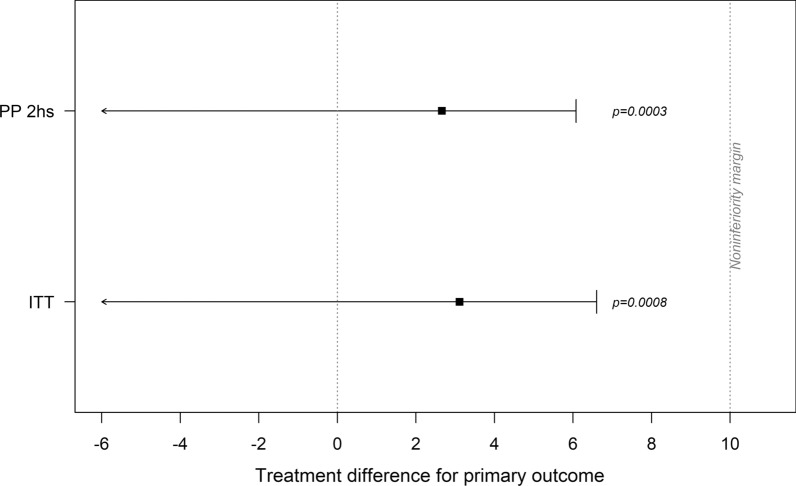
Methods: We performed a multicenter, non-inferiority randomized trial comparing HFNT and noninvasive ventilation (NIV) in nine centers in Italy. Patients were eligible if presented with mild-to-moderate AECOPD (arterial pH 7.25-7.35, PaCO2 ≥ 55 mmHg before ventilator support). Primary endpoint was the mean difference of PaCO2 from baseline to 2 h (non-inferiority margin 10 mmHg) in the per-protocol analysis. Main secondary endpoints were non-inferiority of HFNT to NIV in reducing PaCO2 at 6 h in the per-protocol and intention-to-treat analysis and rate of treatment changes.
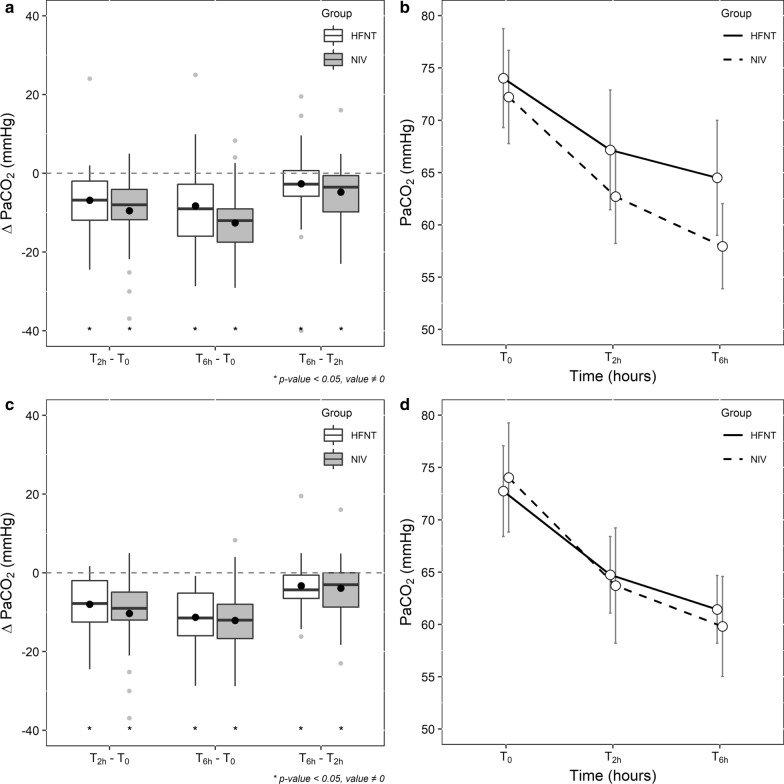
Results: Seventy-nine patients were analyzed (80 patients randomized). Mean differences for PaCO2 reduction from baseline to 2 h were - 6.8 mmHg (± 8.7) in the HFNT and - 9.5 mmHg (± 8.5) in the NIV group (p = 0.404). By 6 h, 32% of patients (13 out of 40) in the HFNT group switched to NIV and one to invasive ventilation. HFNT was statistically non-inferior to NIV since the 95% confidence interval (CI) upper boundary of absolute difference in mean PaCO2 reduction did not reach the non-inferiority margin of 10 mmHg (absolute difference 2.7 mmHg; 1-sided 95% CI 6.1; p = 0.0003). Both treatments had a significant effect on PaCO2 reductions over time, and trends were similar between groups. Similar results were found in both per-protocol at 6 h and intention-to-treat analysis.
Conclusions: HFNT was statistically non-inferior to NIV as initial ventilatory support in decreasing PaCO2 after 2 h of treatment in patients with mild-to-moderate AECOPD, considering a non-inferiority margin of 10 mmHg. However, 32% of patients receiving HFNT required NIV by 6 h. Further trials with superiority design should evaluate efficacy toward stronger patient-related outcomes and safety of HFNT in AECOPD.
Trial registration: The study was prospectively registered on December 12, 2017, in ClinicalTrials.gov (NCT03370666).
Keywords: Acute respiratory failure; Chronic obstructive pulmonary disease; High flow nasal cannula; High flow nasal therapy; Noninvasive ventilation.
Conflict of interest statement
Dr. Cortegiani, Prof. Giarratano and Prof. Gregoretti declare a patent pending, in association with the University of Palermo—Italy (No. 102019000020532—Italian Ministry of Economic Development), not discussed in the present study. Prof. Gregoretti received honoraria for lectures or consultancies from Philips, Resmed, Vivisol, OrionPharma, Origin (not relevant to this protocol). Prof. Enrico Clini received fees for lectures from Chiesi, Astra-Zeneca, Menarini, Guidotti_Malesci, and AlfaSigma (not relevant to this protocol). Prof. Stefano Nava’s institution received unrestricted research grant from Fisher and Paykel. Prof. Paolo Navalesi’s institution received funding from Maquet Critical Care, Draeger, and Intersurgical S.p.A.; he received honoraria/speaking fees from Maquet Critical Care, Orionpharma, Philips, Resmed, Merck Sharp & Dome, and Novartis; he disclosed that he contributed to the development of the helmet Next, whose license for patent belongs to Intersurgical S.P.A., and receives royalties for that invention. Prof. Federico Longhini and Prof. Paolo Navalesi contributed to the development of a device not discussed in the present study whose patent is in progress (European Patent application number EP20170199831). Dr. Paolo Groff received honoraria for lectures from Aspen Pharmaceuticals and Menarini Pharmaceuticals (not relevant to this study). Dr. Luigi Vetrugno received travel support for congress lecture by Cook Medical. The remaining authors have disclosed that they do not have any conflicts of interest.
Figures
References
-
- Singh D, Agusti A, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J Engl. 2019;2019:53. - PubMed
-
- Bruni A, Garofalo E, Pelaia C, Messina A, Cammarota G, Murabito P, et al. Patient-ventilator asynchrony in adult critically ill patients. Minerva Anestesiol Italy. 2019;85:676–688. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
