

Local signs at insertion site and catheter-related bloodstream infections: an observational post hoc analysis using individual data of four RCTs
- PMID: 33317594
- PMCID: PMC7737269
- DOI: 10.1186/s13054-020-03425-0
Local signs at insertion site and catheter-related bloodstream infections: an observational post hoc analysis using individual data of four RCTs
Abstract
Background: Little is known on the association between local signs and intravascular catheter infections. This study aimed to evaluate the association between local signs at removal and catheter-related bloodstream infections (CRBSI), and which clinical conditions may predict CRBSIs if inflammation at insertion site is present.
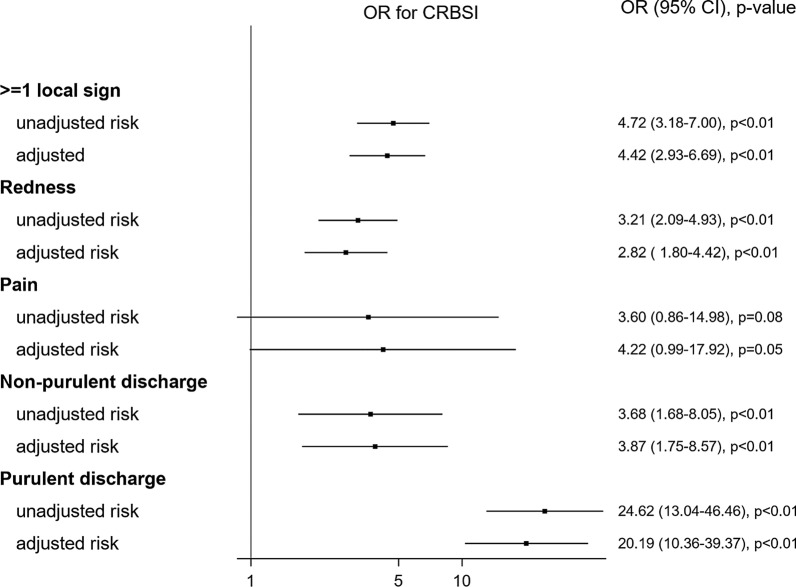
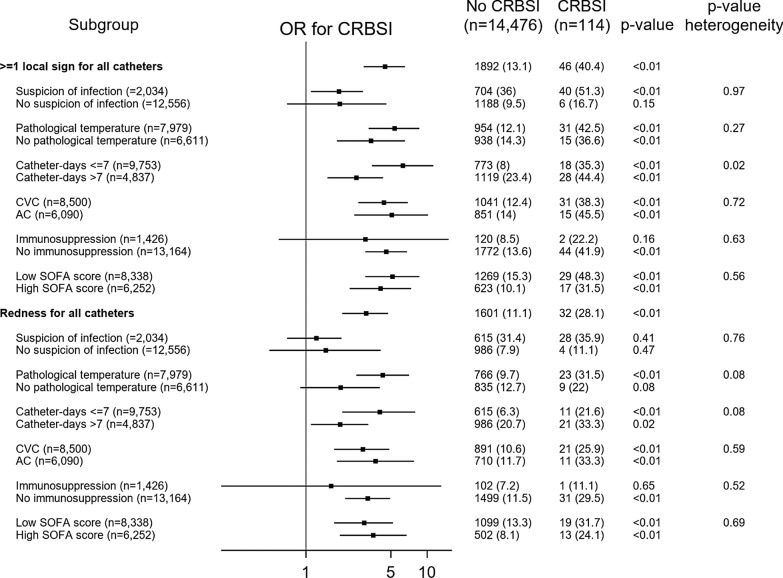
Methods: We used individual data from four multicenter randomized controlled trials in intensive care units (ICUs) that evaluated various prevention strategies for arterial and central venous catheters. We used multivariate logistic regressions in order to evaluate the association between ≥ 1 local sign, redness, pain, non-purulent discharge and purulent discharge, and CRBSI. Moreover, we assessed the probability for each local sign to observe CRBSI in subgroups of clinically relevant conditions.
Results: A total of 6976 patients and 14,590 catheters (101,182 catheter-days) and 114 CRBSI from 25 ICUs with described local signs were included. More than one local sign, redness, pain, non-purulent discharge, and purulent discharge at removal were observed in 1938 (13.3%), 1633 (11.2%), 59 (0.4%), 251 (1.7%), and 102 (0.7%) episodes, respectively. After adjusting on confounders, ≥ 1 local sign, redness, non-purulent discharge, and purulent discharge were associated with CRBSI. The presence of ≥ 1 local sign increased the probability to observe CRBSI in the first 7 days of catheter maintenance (OR 6.30 vs. 2.61 [> 7 catheter-days], pheterogeneity = 0.02).
Conclusions: Local signs were significantly associated with CRBSI in the ICU. In the first 7 days of catheter maintenance, local signs increased the probability to observe CRBSI.
Keywords: Catheter-related bloodstream infection; Exit-site; Insertion site; Intravascular catheter; Intravascular catheter infection; Local sign.
Conflict of interest statement
The authors have disclosed that they do not have conflict of interest. JFT received fees for lectures to 3M, MSD, Pfizer, and Biomerieux. JFT received research grants from Astellas, 3M, MSD, and Pfizer. JFT participated to advisory boards of 3M, MSD, Bayer Pharma, Nabriva, and Pfizer. OM received fees for lectures for 3M and BD. OM received research grants from BD.
Figures
References
-
- ECDC. Healthcare associated infections acquired in intensive care units - annual epidemiological report for 2016. Stockholm (Sweden): European Centre for Disease Prevention and Control; 2018. https://www.ecdc.europa.eu/sites/default/files/documents/AER_for_2016-HA.... Accessed 3 Oct 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
